
Dr. Robert Clancy writes at Quadrant We Can’t Vaccinate This Pandemic Away. The author is Emeritus Professor of Pathology at the University of Newcastle Medical School. He is a member of the Australian Academy of Science’s COVID-19 Expert Database. Excerpts in italics with my bolds.
Thirty frontline doctors in Australia recently treated over 600 patients with COVID-19. The treatment strategy was ivermectin (IVM) with doxycycline and zinc. Five patients required admission to hospital for progressive symptoms. There were no deaths. In a similar number of contemporary Australian patients not treated with IVM, 70 were hospitalised and six died. See Ivermectin Proven Successful in Australia
This is consistent with world data bases: 31 randomised controlled trials show 62 per cent benefit with IVM, and seven meta-analyses recorded a reduction in death of between 57 and 83 per cent. Experienced clinicians have moved on to combine IVM with additional drugs, usually a broad-spectrum antibiotic such as doxycycline, and zinc, which has viricidal activity.
A logical conclusion would be that these results demand attention. With “freedom day” in NSW expected to be followed by increases in COVID-19 infections and hospital admissions, an IVM roll-out would be a logical outcome. That this has not happened may well prompt the question ‘Why is that so?’ The mainline press, which continues in its refusal to report and interrogate the evidence, also fails the public by presenting IVM as the antichrist of the medicine cabinet. A complex set of events has come together. These events and how they affect COVID-19 management and patient outcomes form the basis of this article.
1. Bureaucrats Usurped Medical Choice from Doctors and Patients
FIRST, as patients were being treated with IVM in Sydney and Melbourne with the impressive results mentioned above, the Therapeutic Goods Administration (TGA) made an extraordinary move to shut down the prescribing of IVM by frontline doctors for the treatment and prevention of COVID-19. The TGA has form, as it made a similar ruling on hydroxychloroquine (HCQ), the other re-purposed off-patent drug shown to be effective in treating COVID-19. Importantly, the reasons given by the TGA to justify its decision were not correct.
The main TGA concern stated was that IVM would confuse the public and lead to hesitation to be vaccinated. That, too, is incorrect. Doctors overwhelmingly support vaccination against COVID-19. The combination of safe and effective IVM with a vaccination programme will enhance viral clearance, reduce disease severity, reduce hospital admissions and reduce deaths. However, groupthink quickly led to professional bodies such as the AMA uncritically accepting the TGA policy. Even the Australian Academy of Science weighed in with political support for the TGA’s decision, doing so without any evaluation of the science.
Then came the coup: the regulatory body responsible for registration of doctors, the Australian Health Practitioner Regulation Agency, warned that prescribing, dispensing, or even publicly discussing IVM, “compromised expected standards of practise”, leaving open disciplinary measures which have since resulted in doctors having their licences revoked. A crescendo of intimidation has ensued, all based on a failure to interrogate the data and understand the clinical circumstance, with perhaps a touch of group hysteria thrown in.
The conclusion to be taken from these collective authoritarian decisions is that medical choice is no longer the prerogative of the doctor-patient relationship in Australia. Bureaucrats for any reason can decide and enforce medical issues without discussion with relevant medical experts. This is a problem throughout the Western world, but perhaps there is a light in the tunnel. Nebraska’s attorney general recently ruled that the prescription of IVM for COVID-19 is a matter for the doctor and patient, not government. See Nebraska AG Frees Doctors and Patients to Use HCQ and IVM
2. Evidence for Early Treatment is Stronger and Critiques Discredited
THE SECOND development is a changing balance in evidence relevant to early treatment. Negative critique has been rebutted, and support has become stronger.
First, there has been a rebuttal of a misleading “Cochrane report“. Traditionally, a Cochrane is considered the highest bar for drug efficacy, and the outcome of a Cochrane has profound influence on acceptance. The existing Cochrane report on IVM was ambivalent. . . Recently, a group of respected non-aligned epidemiologists in the UK reviewed the Cochrane report and found it wanting. They showed defects in method, an exclusion of data points and studies, and a failure to include substantive regional and national experiences where IVM had been successfully adopted.
Not to be dismissed, IVM naysayers took a new tack: play the man (or the woman), not the ball. Their trick is to label IVM studies that do not fit their viewpoint as “fraudulent” while disparaging IVM’s medical supporters as, among other insults, “New Age quacks”. The value of the naysayers’ critique, indeed their motivation, has been challenged in detail (see IVMMETA.com), failing on numerous counts that include an absence of evidence and misinformation.
The mainline press welcomed claims supporting the anti-IVM narrative, with the BBC News plumbing new lows in journalism by combining false conclusions with bias that included misrepresentation of a highly regarded epidemiologist. A recent Sydney Morning Herald article was little better, distorting the science with ideology and bias. The reporter involved has not responded to a request to host a debate on the topic. They never do!
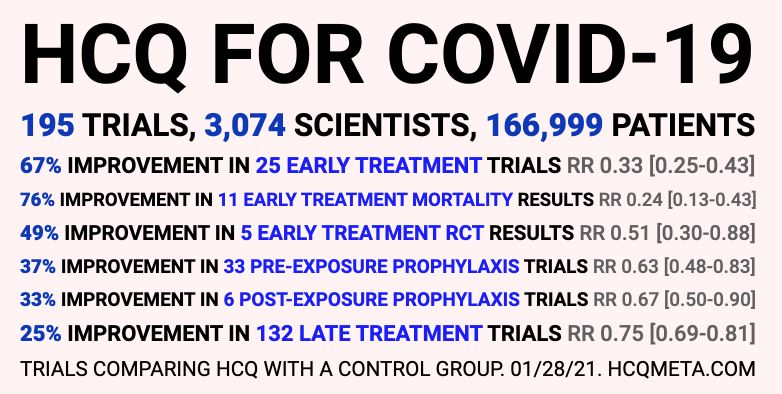
Second, and more positive, is the accumulation of evidence supporting the benefit from early treatment. Two recent and compelling studies further support the value of both IVM and HCQ , the latter having been “cancelled” after being cited by Donald Trump as a potential treatment. All this came despite a meta-analysis of 32 early-treatment studies showing 64 per cent protection.
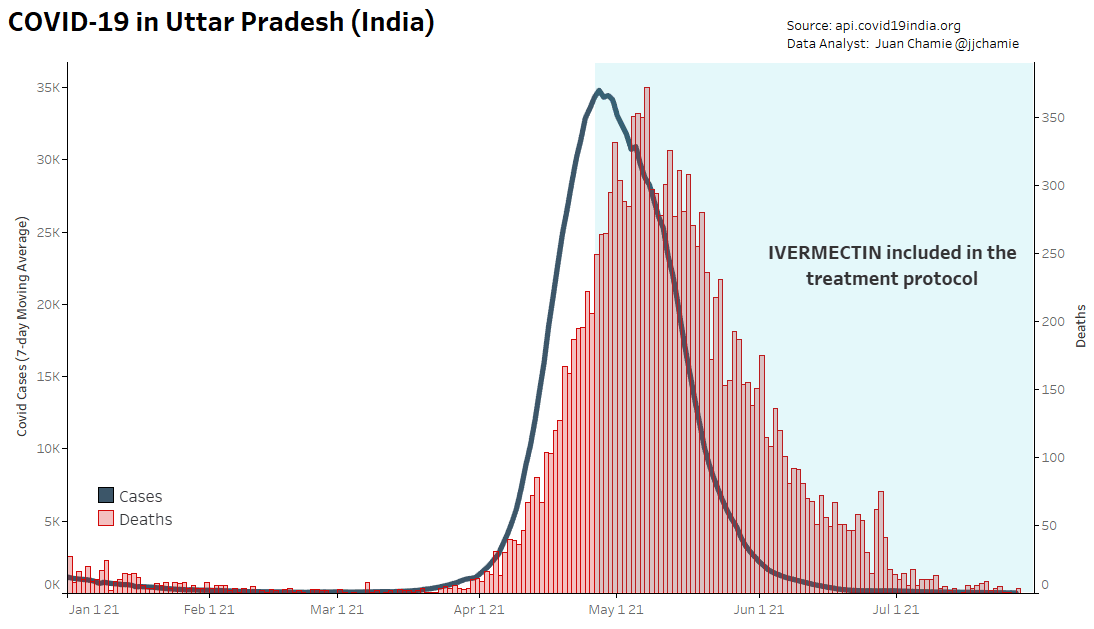
The first of those is a WHO study in Uttar Pradesh, India’s most populous state (230 million people). Medical teams visited 98,000 villages, providing kits (similar to those used in the Australian study) containing IVM for the treatment of those with COVID-19. Within five weeks, new cases had dropped by 97 per cent. Meanwhile in another Indian state, Kerala, with eight per cent the population of Uttar Pradesh, IVM was not used and as many as 31,000 COVID cases were recorded per day. Similar results are reported in areas of Peru, Mexico and elsewhere.
The second recent study treated 8,300 French patients with HCQ. There was a 93 per cent reduction in mortality. A meta-analysis by the same authors included 32,000 patients from five countries and showed early HCQ treatment reduced mortality by 69 per cent.
The inevitable and unavoidable conclusions to be drawn are that Cochrane negativity can no longer dominate an honest argument about IVM’s use and, further, that the medication must be accepted in Australia as a safe and effective treatment capable of reducing the expected post-lockdown load on health systems.
3. Merck Pill is Inferior IVM Substitute: Less safe, less effective and Expensive
THE THIRD development has been the frenetic response by media and government to an orchestrated campaign by pharmaceutical giant Merck promoting its re-purposed antiviral agent, Molnupiravir, before significant data assessment has been completed. Merck is now joined by Roche and Pfizer with their versions of re-positioned “wonder drugs”. All have limited and conflicting data yet make extravagant claims. These antivirals are less effective than IVM and none have acceptable safety profiles. However, we see the Australian government making extraordinary claims and committing large sums to acquire these unproven oral therapies.
Who can be advising government to allow such dubious claims and acquisitions at the expense of IVM and the Australian taxpayer?
The charge of hypocrisy and cynicism must first be directed at Merck, but also at “the experts”, Dr.Tony Fauci, governments and, of course, the media. Merck stated IVM had no clinical value mere days before receiving a US$300 million grant to develop Molnupiravir. Available data suggests it provides eight-fold less protection than that found for IVM in the Australian study. Merck acquired Molnupiravir, originally developed by Emory University, after it failed against other RNA virus diseases. Questions about undisclosed data remain to be answered. The drug is a “son of Remdesavir”, a RNA polymerase inhibitor that failed randomised controlled trials (RCT). The Australian government has bought 300,000 courses of Remdesivir (the US government pays US$1,000 per course). This is beyond logic, certainly not based on science. As the TGA prevented doctors prescribing IVM because it would reduce vaccination rates, the question is simple: How will the TGA draw a distinction between Merck’s Molnupiravir and IVM?
The elephant in the room for Molnupiravir is safety. The drug creates lethal mutants to terminate virus replication. Cell biologists express concern that some live mutants with resistance to vaccines are released into the environment. DNA mutations also occur, which could lead to disturbed growth and cross-generation transmission of genetic changes.
The TGA will now have to wrestle with pressure from Big Pharma and government to register a drug with scant clinical data and untested safety concerns after denying the Australian public a cheap, safe and more effective treatment with IVM.
4. Realizing the Limitations of Genetic Vaccines
THE FOURTH issue is the recognition that genetic vaccines have limited value. While doctors support the current vaccine roll-out, reported “danger signals” must be clarified. Both the DNA-vector vaccine (AstraZeneca) and mRNA vaccines (Pfizer and Moderna) behave as predicted by biology relevant to airways’ protection (something not understood by the vast majority of “experts”): short duration of protection limited to control of systemic inflammation, with little impact on infection of the airways.
Israel was used as a laboratory for the Pfizer vaccine. Six months after vaccination, there was essentially no protection against infection or mild disease, although protection against severe disease remained at 85-to-90 per cent. Thereafter came a rapid and progressive loss of protection against more severe disease. Infected vaccinated and unvaccinated subjects have similar viral loads and transmission capacity. Immunity following natural infection is better and more durable than that induced by vaccination, so there is no sense in immunising those who have had COVID infection in the preceding six months.
In an Australian context, by New Year 2022, it is estimated about two million vaccinated Australians will have lost protection against infection and mild disease. Infections will increase as borders are opened and we re-enter the international community.
Our lockdown policy has limited the acquisition of natural immunity. Although we can expect high levels of infection with less severe disease, pressure on hospitals will increase. The experience of Israel and Iceland, each with high vaccination rates of 85 per cent or more, provides a possible scenario for Australia. In Israel, with a population of less than 10 million, the “third wave” continues, with 1500 new cases and 30 deaths a day (at the time of writing). More concerning are reports of high COVID mortality in older vaccinated subjects in some jurisdictions. Variants such as the further-mutated Delta variant in the UK will continue to appear, with unknown infectivity, response to current vaccines and pathogenicity. Perhaps of greatest concern is the observation in the UK, and now in Sweden, that older vaccinated individuals have a higher incidence of COVID infection than those who are unvaccinated. At the same time others are describing a state of immune deficiency following vaccination with genetic vaccines.
At this stage it is unclear as to whether this “deficiency” of the immune response is limited to the antibody response to COVID virus. This should not be a surprise to anyone who has done “Immunology 101”, as enhancing antibody (ie antibody that promotes infection, rather than limits it) is well recognised in RNA virus infections, and “antigen excess causing a downregulation of immunity” is a basic tenet of immunology. Forgotten by most, is that genetic vaccines cause a large and unregulated amount of antigen (ie the spike protein) to be synthesised within the cells of the body, and the immune response will be a function of those unknown dynamics. These facts and the concerns they raise should be front and centre for regulators as they examine data to make decisions in regard to booster shots. The duration of protection following boosters is completely unknown, as is whether genetic vaccine boosters distort the immune system with net suppression. Are we setting ourselves up for monthly boosters, higher incidence of infections, more serious adverse events, or even more concerning immune outcomes. We just do not know!
If ever there was a need for a safe , cheap effective oral therapy, now is it.

Protocols including IVM or HCQ + nutrients fill the need for early home treatment.

Basically same stats as other flus. Wow! I explained that much faster..
LikeLike
Not so fast dw. The flus are contracted and transmitted mostly by children, and some of them get sick (a very few die). This coronavirus is a risk mostly to the elderly who are already battling one or more deadly diseases. Children have a higher risk of covid vaccine side effects, then their chances of catching the virus itself (even then they beat CV19 easily). And now with the variants, even adults have more chance of a runny nose, but less chance of serious illness. Still, for safety’s sake, everyone should have access to anti-viral home treatment medicines, as Dr. Clancy recommends.
LikeLike
I get from my simple reply, you saw me standing there, like one waiting for an education. Nope. Did the homework. Observed. Listened to doctors, also reading between the lines. Read some bloggers, then read statistics, of course, that has it’s own level of complexities due to politics. But I talk this way because I don’t ever trust intellectuals who attempt to sound intelligent, but don’t truly demonstrate knowledge. You might be a rare one who actually is doing homework, but slanted by your own proclivity to believe, and that’s okay, but we hope you continue to research. As far as the trends and stuff, I seriously doubt real information sources put together with such revelations. More like polar bears swimming off ice when they’ve always done so, to prove ice is melting. Polar bears love swimming.
LikeLike
Lighten up, please.
LikeLike
You wrote an article purporting to be serious, and I addressed it as that. There are readers who fall for such things and need to see responses of understanding. Of course, I wrote that while having a nice cup of cocoa, having gone fishing that day. Pretty relaxing. You enjoy your day.
LikeLike
Your comment was flippant and dismissive. I responded with reasons why the article was relevant. Thanks for disclosing that you already know it all, and have no respect for others’ information. Please enjoy your trolling elsewhere.
LikeLike
Thanks for the article and statistics on effectiveness of Ivermectin in Covid 19 patients. Eventually the truth will win as more people are informed.
LikeLike
Reblogged this on HiFast News Feed.
LikeLike