Recently Dr. Robert Malone was interviewed at length by Joe Rogan and the full transcript is Joe Rogan Experience #1757 – Dr. Robert Malone, MD Full Transcript
Below are excerpts in italics with my bolds, lightly edited and rearranged to serve as a synopsis. Read the full transcript for more details and technical points.
For about the last 20 years I’ve been focused on actually doing stuff: regulatory affairs, clinical development, getting necessary training, etc. I also completed a fellowship at Harvard University medical school as a global clinical scholar to round out my cv. And I’ve run over 100 clinical trials, mostly in the vaccine space, but also in drug repurposing. I’ve been involved in every major outbreak since AIDS. This is kind of what I do. I’ve won literally billions of dollars in federal grants and contracts. I’m often brought in by NIH to serve as a study section chair for awarding 80 to 120 million dollar contracts in vaccines and biodefense.
So, my position all the way through this comes off of the platform of bioethics and the importance of informed consent. People should have the freedom of choice particularly for their children; and in order to appropriately choose to participate in a medical experiment, they have to be fully informed of the risks as well as the benefits. And so I’ve tried really hard to make sure that people have access to the information about those risks and potential benefits, the true unfiltered academic papers and raw data etc. However, the policy that’s being implemented is one in which no discussion of the risks are allowed because by definition they will elicit vaccine hesitance. So it can’t be discussed, and yet that’s the backbone of informed consent. So not only is informed consent not happening, it’s being actively blocked, which makes no sense.
Michael Callahan is a CIA agent that I’ve co-published with in the past. He was in Wuhan in the fourth quarter of 2019 and he called me from Wuhan on January 4th, 2020. was currently managing a team focusing on drug discovery for organophosphate poisoning, ergo nerve agents for DTRA, defense threat reduction agency. It involved high-end stuff like high-performing computing and biorobot screening. And he told me, Robert you need to get your team spun up because we got a problem with this new virus. I worked with him through prior outbreaks, and so it was then that I turned my attention to this. We started modeling a key protein, a protease inhibitor of this virus when the sequence was released on January 11th as the Wuhan seafood market virus. And I’ve been pretty much going non-stop ever since to address that outbreak with drug repurposing.
I’ve got some good news to announce. Today we should have the first patient enrolled in our clinical trials of the combination of monitoring and celecoxib for treating SARS-CoV-2. These trials are being run by the company Leidos, which is one of my clients. I’ve helped them design a plan based on my discoveries and funded by a defense threat reduction agency. I haven’t pushed this drug combination feeling it was inappropriate until we got the trials running. But they’re now open and we’ve passed through the FDA screening process. We had data showing that adding Ivermectin would further improve the combination, but the FDA created such enormous roadblocks to us doing an Ivermectin arm that we had to drop it. And by we I mean the DOD decided the juice wasn’t worth the squeeze, and they just dropped that arm due to FDA creating so much grief.
There are good modeling studies that probably half a million excess deaths have happened in the United States through the intentional blockade of early treatment by the U.S. government. it’s the pushback against both Hydroxychloroquine and Ivermectin now. When you ask me why, you’re asking me to get into somebody’s head. What I can say as a scientist is what I observed: the behaviors, the actions, the correspondence, these bizarre things that have happened.
For example, it is well documented they conspired to cook up a strategy using emergency use authorization to make it so that Hydroxychloroquine could only be administered in the hospital, which is too late for when hydroxy should be used. The government had documents on hydroxy’s safety and effectiveness yet they asserted that there was no data on Hydroxychloroquine at the time this decision was made. Just patently false. So, what is the motivation when none of this makes sense? The only thing you know is this is a journalist problem, and you know the classic guidance is follow the money.
And it is bizarre that Merck would come out with these explicit statements about the safety of Ivermectin. Both Ivermectin and hydroxy are on the WHO list of essential medicines. They have been administered for millions and millions of doses; they’re among the safest known medicines when administered within this acceptable pharmaceutical window. Ivermectin is even safer than hydroxy, so Merck coming out of the blue and saying Ivermectin isn’t safe is really inexplicable.
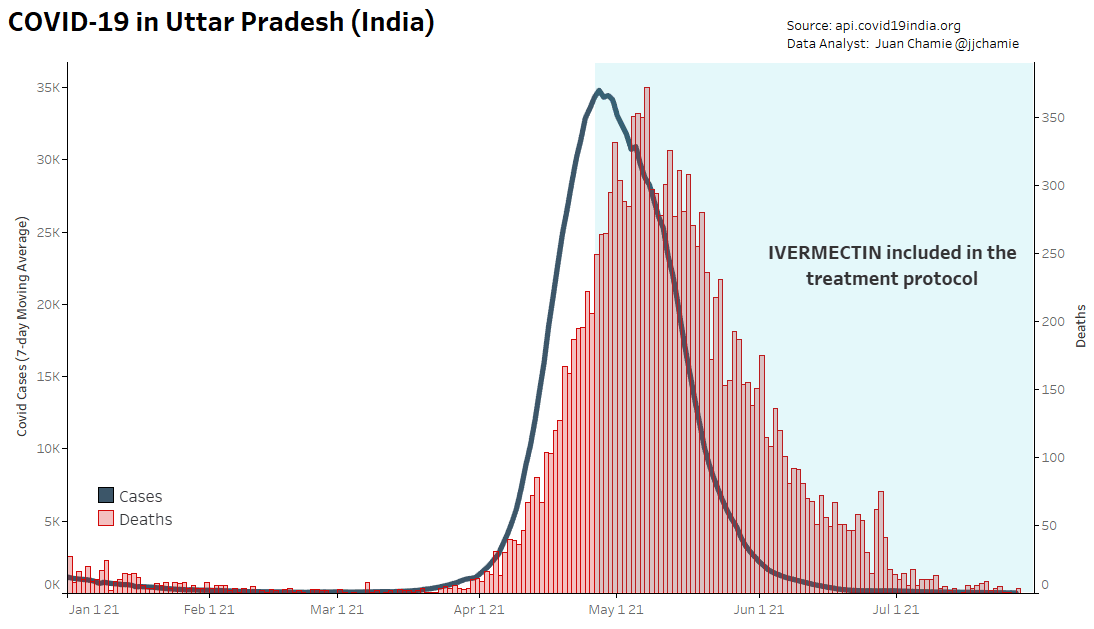
In India, Uttar Pradesh has almost the same population as the United States; it’s huge, dense, urban and poor, all the characteristics of the Indian countryside. And the virus was just ripping through there, causing all kinds of death and disease. Out of desperation it was decided to deploy widely throughout the province early treatments as packages including a number of agents. The composition has not been formally disclosed but it was rumored to include Ivermectin. There was a specific visit of Biden to Modi, and thereafter a decision was made in the Indian government not to disclose the contents of those packages that were being deployed in Uttar Pradesh. The treatments are still in use there, and in Uttar Pradesh deaths have flatlined. The rest of the world is yelling about Omicron and about hospitalizations–well South Africa isn’t–and Uttar Pradesh is still flatlined in terms of deaths.
The observation that I can make if we follow the money is that hospitals are incentivized to to treat COVID patients. The thing that ties all this together, including the suppression through the government of early treatment, is hospitals are incentivized financially to treat COVID patients. For example, in the Imperial Valley of California, COVID patients are being treated outside of the hospital and prevented from going to the hospital. Brian Tyson and George Fareed have saved thousands and thousands of lives of indigenous Latinos that are coming across the border and working the fields. I mean they’re they’re breaking their backs to save the poor, an amazing story there with early treatments. I guess they’re left alone because they’re in the imperial valley nobody cares, they’re all poor, but in these urban environments there’s all these incentives for hospitals to treat COVID patients and if people are giving treatments that are keeping those people out of the hospitals then they’re not getting that revenue. Hospitals have financial incentives including death incentives to discourage early treatment. The other data point is those that are doing the attacking are almost universally hospital administrators and hospitalists, I.e. hospital-based physicians
I’m maybe the only one that has been involved deeply in the development of this tech that doesn’t have a financial stake in it, so for me the reason is that what’s happening is not right. It’s destroying my profession; it’s destroying the practice of medicine worldwide; it’s destroying public health in medicine. I’m a vaccinologist, I’ve spent 30 years developing vaccine, a stupid amount of education learning how to do it and what the rules are. And I’m personally offended by watching my discipline get destroyed for no good reason at all except apparently financial incentives, and perhaps political ass covering.
We have Covid mRNA genetic vaccines, and we have DNA virus administered genetic vaccines (that’s the J&J here in the United States). And they all have these symptoms of clotting, brain fog and other things. As you know this is basically: Does it walk like a duck and quack like a duck? What is the common variable between those three very different systems: natural viral infection, mRNA genetic vaccines, and DNA genetic vaccines? We don’t see these problems by the way with adenoviral vectored vaccines in development for my entire life. 30 years they’re licensed, adenoviral vector vaccines they don’t have these problems, so it’s something that’s not intrinsic to the platform. The common variable is spike protein just to cut to the chase.
Then then there is this fundamental logic flaw. In clinical development and non-clinical development and safety and pharmacology, I like to say the French judicial system applies. That is, you’re guilty until proven innocent. It’s the job of the pharmaceutical companies to prove that their engineered spike is safe. They never did that. And so all of this pressure that comes back you know from folks like me saying hey this isn’t right okay–and it looks like a duck and it walks like a duck and it quacks like a duc–it’s probably toxic. Because it’s the common variable. I get criticized by people saying you have to prove that it’s not safe. Sorry, that’s not the way it works. It’s pharma’s job to prove that it is safe, not my job to prove that it’s not safe. I’m observing the safety signal is there. It is associated with vectors that express spike whether it’s the vaccine the virus or the adenovirus, that is the MRNA, the virus itself or the adenoviral vectored spike. Those toxicities are there and the common variable is the spike protein. We can argue about the meaning of toxin just like so much of the rest of our language has been perverted during this. But the simple explanation, the simple definition is: Does it cause toxicity in people, and the answer is pretty clear now it does. The question that we’re all arguing about is how often and how bad.
Then we have the laboratory data that we’re seeing abnormalities in the key signaling molecules that b and t cells use to talk to each other–toll-like receptors that are associated particularly with the MRNA vaccines. So something is happening that is causing release of t cell suppression, reactivation of latent DNA viruses, maybe some signals relating to oncology, that is some changes in t cell signaling behavior. And then there’s this this increasing awareness that there’s some window of time, unsure how long after vaccination, when you’re actually more susceptible to infection. And this may be that not only is the vaccine efficacy waning, but the multiple jab strategy is actually creating more and more windows where people have this period of t-cell suppression. So there’s a whole lot in this box of immunology and what are the jabs doing to our immune system and how long does it last. Let’s gently say: That is a little worrisome to some of us that have a background in these things.
In this case there’s multiple reasons not to do the multiple jabs. The simplest one for everybody to understand is when your son develops seasonal allergies to ragweed pollen or whatever and it’s so bad that he can’t go to school his eyes are running he can’t play in sports whatever. So you say we have to do something about this: I’m going to take him to a rheumatologist an allergist and see what they can do. Well they do a bunch of tests and they say oh your son is allergic to ragweed pollen or whatever the thing is. Then what do is to give him shots- what are those shots? They’re high doses of antigen that are administered repeatedly to your child, and what it does is induce something we immunologists call high zone tolerance. High zone tolerance basically amounts to an ability by giving multiple injections at high levels of antigen to shut down t cells against a specific antigen. The other thing with the multiple jabs is that these are multiple jabs that are mismatched. Okay they don’t fit.
So there’s there’s those three things. The short term issue is we don’t know how long it lasts. There’s the high zone tolerance issue, and then there is the multiple jabs that are mismatched for the current circulating virus. That’s akin to repeatedly taking a flu vaccine from two seasons ago and hoping it’s going to protect against this flu.
So what we’re doing is with with administering a mismatched vaccine is we’re driving the effector and memory cells, b and t, towards a population that is focused on a virus that no longer exists. So what is my hypothesis for the poor durability of the vaccines? My answer is it looks to me like original antigenic sin. Let’s unpack what that terminology means–original antigenic sin. I think what could be happening with these data is that we’re driving the immune response towards responding to an antigen receptor binding domain a spike that no longer exists with Omicron. Now it it has become clear (after being initially denied) that all of us have a background immune response against Beta coronaviruses. These are naturally circulating cold coronaviruses that have significant immunologic crossreactivity with SARS-CoV-2. And the problem with that in original antigenic sin is that those existing memory cells will dominate the immune response when you get infected and when you get vaccinated. Let me unpack that in a way that kind of makes sense for the common person. We all know the adage that we’re always best prepared for the last war. That is, in your life the sum of your prior life experiences biases how you respond. In your martial arts you must know this deeply; what you’ve experienced in the past in prior fights is gonna bias how you respond to a new opponent. Same thing happens with your immune system.
Okay so we’ve got a new pathogen, but it’s got a series of of overlaps with the old ones that we’ve seen before, and our immune system is biased to respond as if it’s the old one. Now to make matters worse, we’re taking the spike protein only one of the proteins–the immunologically dominant protei–and we’re jabbing everybody multiple times. Thereby driving memory cells and effector cells to a virus that is not the one we’re encountering. So it could very well be that as you’re taking more jabs you’re further skewing your immune response in a way that’s dysfunctional for infection to Omicron. Whereas, somebody that is immunologically naive presumably either they haven’t had the virus before but they’ve had Beta coronaviruses and those that have had prior infection and are naturally immune.
When you get infected or I get infected it’s typically nasal or oral pharynx. It’s coming in through the mucosal membranes of your head. One of the good things about Omicron is that the prior strains infect mostly deep lung, and there’s really fascinating data from Hong Kong suggesting that Omicron is more infecting the upper airway. That is a characteristic of less pathogenic influenza viruses and hopefully even though Omicron is more infectious and replicates the higher levels it’s less pathogenic.
it is absolutely looking like Omicron is a mild variant. It is absolutely able to escape the control of prior vaccination typically with mismatched vaccine. It seems also able to infect a subset of people that are naturally immune probably less than the subset that get infected with vaccination. But this is a key message to your audience- the reproductive coefficient (more fancy language)–the reproductive coefficient known as the R naught. The R naught of the original Wuhan strain was about two to three, meaning that if I’m infected on average without any other interventions I’ll infect two to three other people. For Delta the R naught was more in the range of five to six. In the case of Omicron the R naught the base reproduction coefficient is the range of seven to ten, wickedly high. That is measles territory. Tto translate that into simple language: We are all going to get infected with Omicron. Whether you use masks or not, use social distancing or not, you’re going to get infected. So this gets to the key point: Find a doc that’ll administer early treatments.
So you know Joe Lapado surgeon general in the State of Florida has put out public statements also on twitter, among other things, decrying what the Federal government has done pulling back all of the regular monoclonals. Meanwhile I’m hearing from frontline docs is those older regeneron monoclonals etc. are still very effective in their hospitalized population presumably because it’s still predominantly Delta. And yet they’re no longer able to get it. So the government has literally stopped the distribution of medicine, effective medicine, for a disease that exists currently. When has that ever happened before? Hydroxychloroquine and ivermectin. Those were off-label uses, while this is something that has emergency use authorization. This is wild.
When you see this kind of decoupling of public policy from logic, it causes thinking people to wonder what the hell’s going on here. And then we go down the rabbit hole: Is it this that or the other thing? One of the things in that spectrum of what’s going on is that the emergency use authorizations are predicated on policy determinations that were in a state of emergency. Those are now two years old. They’re expiring. I’m not saying this is what’s going on in their head but there is another perverse incentive here to amplify the fear porn. If you buy into the hypothesis that for some reason there are incentives for the government to maintain the state of emergency, one explanation could be that those declarations are expiring and will have to be re-implemented. Because if they’re not then all of this emergency use authorization vanishes like dust.
We have these reports from hospitalists and nurses–often it’s the nurses that are able to speak for some reason. The nurses are disclosing things that they’re seeing in their hospitals and the physicians are all shutting up. Is it because they have financial incentives or because they’re all owned because they have such debt burdens, I don’t know. But the nurses are speaking out and they’re saying hey we’re seeing strokes and heart attacks and these other types of problems that are known to be associated with the jabs. Well it’s hard to say because we got the virus in the vaccines overlapping; is it chicken or egg but we know that they’re happening. We know that the deaths are happening; that’s the excuses that are made about the sudden deaths in high-performing athletes that are being observed all over the world particularly in footballers. Where they’re just suddenly dropping is it because they’ve been infected or they because they’ve been jabbed? And I think it’s a mixture of both. But the thing about the vaccines is we have this principle to do no harm. And if a virus naturally infects you and you have a damage from it, I haven’t caused that damage as a physician. If I’m recommending that you take a drug or an intervention you didn’t need to have and it causes damage, well I have to own that as a physician as a representative of the medical industrial complex. And so for whatever reason there’s a under reporting bias clearly in the adult population and I think that people being be a little more sensitive to adverse events and deaths in their children.
I don’t want to get too off your topic, but our government is out of control on this and they are lawless. They completely disregard bioethics. They completely disregard the Federal common rule. They have broken all the rules that I know of that I’ve been trained on for years and years and years. These mandates of an experimental vaccine are explicitly illegal. They are explicitly inconsistent with the Nuremberg Code. They’re explicitly inconsistent with the Belmont Report. They are flat out illegal and they don’t care. And the only thing standing between us and it’s too late for many of our colleagues including my you know the unfortunate colleagues in the DoD um hopefully we’re going to be able to stop them before they take our kids.
For example: the lab leak. And for me- the disclosure of emails that um Cliff Lane, Tony Fauci, and Francis Collins actively conspired to destroy any discussion of the appropriateness of lockdown strategies and the mainstream press hardly covers it and there are no consequences. The document trail having to do with the gain of function research and the implication of NIH and by the way DTRA in that, having absolutely no consequences for anybody. We’re in an environment in which truth and consequences are fungible. This is modern media management and warfare. The truth is what those that are managing the Trusted News Initiative say it is.
And they’re taking our licenses and license to practice medicine because we are speaking about these matters. You can label me however you want, I don’t care. I’ve done what I’ve done in my career. I’m at a stage at 62 years old; I’ve got a farm it’s almost paid off, I raise horses, I love my wife, been married a long time, my kids are both married, I have grandkids, you know I don’t need this. There’s this claim I’m doing all this because I seek attention- trust me this is not a fun thing to be doing at this stage. Physicians at FLCCC in senior positions highly, like Peter Mccullough, people at the at the culmination of exceptional careers. Paul Merrick an exceptional physician by any standards- run out of his hospital demeaned destroyed, actively attacked trying to take his license. This medicine is being destroyed globally. People are losing faith in the whole system. They’re losing faith in the scientific enterprise. They’re losing faith in our government. They’re losing faith in the vaccine enterprise. What is going to be the long-term consequences of public health when you have a large fraction of the population who previously wasn’t anti-vaxxer (that pejorative), but now they’re saying oh my god if this is how these people make decisions I don’t want anything to do with it. I certainly don’t want to jabbed into my kid.
Pfizer is one of the most criminal pharmaceutical organizations in the world based on their past legal history and fines. What do those fines include? Bribing physicians okay, it is a cost benefit analysis in the pharmaceutical industry about misbehavior. They are not grounded in the ethical principles that you and I as average people believe in. They don’t live in that world. As you appropriately point out they are about profit- return on investment. And furthermore the overlords that own them BlackRock, Vanguard, State Street etc. these large massive funds that are completely decoupled from nation states, have no moral core–they have no moral purpose. Their only purpose is return on investment. And that is the core problem here. That and the fact that we as a society have become grossly fragmented through social media, electronic appliances, the stress of what we’ve experienced, and this leads into this whole issue of mass formation psychosis that Matthias DeSmet at the university of Ghent has described, as a psychologist and statistician. That is how a third of the population basically is being hypnotized and totally wrapped up in whatever Tony Fauci in the mainstream media feeds them whatever CNN tells them is true.
Now there’s ways to get out of it. Matthias’s recommendation is you have to get people to realize we’ve got a situation of global totalitarianism. In his experience in Europe making people realize there’s a bigger threat than the virus can cause a separation psychologically in this fusion. This hypnosis that has happened the problem is then you’re just substituting a bigger boogeyman for the current one and somebody else can come in and manipulate that. The real problem and it gets back to your core point- we’re sick as a society and we have to heal ourselves and one of the things we have to do is come together we have to recreate our social bonds, we have to buy into integrity, the importance of human dignity, and the importance of community. That’s how we get out of this and I think that this insight of Matthias Desmond is really central to kind of making sense of all of this crazy. We got a world in which the press is incentivized to push a storyline because they’re all controlled by the same large funds that Pfizer is and so is tech. I don’t know how we’re going to get out of it but it’s got to start with us all of us finding common ground.

That was a brilliant interview. Shame debate has been outlawed the past few years.
LikeLike
“Matthias Desmond at the university of Ghent”
That’s “Matthias DeSmet.” People won’t find Mattiash Desmond anywhere if they search.
And “anagenic sin” should be “antigenic sin.”
LikeLike
Thanks. Fixed.
LikeLiked by 1 person
Cool! I wish more people had listened to the interview before passing judgement!!!!
It’s a long interview, almost three hours. I listened to it in three parts, there was so much discussed!
Thanks for putting it online! VR
LikeLike
Thanks VR. I sent you an email at your website email address.
LikeLike
I got it, sent you back a reply, did you get it? VR
LikeLike