Buzz Hollander MD writes at Real Clear Science Let’s Stop Pretending About the Covid-19 Vaccines. Excerpts in italics with my bolds and images.
As a family physician, I spend my days dispensing advice. I mean, there’s the occasional cast, skin biopsy, or shot, but most of my patients are seeing me for medical counsel. Never have I been asked about one subject so much as the Covid-19 vaccines, and never have I seen so much doubt and confusion among a group of smart, well-educated people. Interpreting the reality of the effectiveness of these vaccines is complicated: it is waning with time, weakened against delta, unknown when coupled with prior infection, and may not be improved with a booster – but there is new, often murky, data emerging every day. Speaking the truth about the vaccines, however, should not be that hard.
We have to be willing to adapt to new data, even when it does not fit neatly into prior messaging.
That’s where our institutions went astray. I understand the desire of our public health officials, spearheaded by the CDC, to instill confidence in the Covid-19 vaccines; they remain the most expedient path to minimize the suffering inflicted by this pandemic. However, by taking on the role of no-nuance vaccine cheerleaders, they left everyone in a worse situation.
Patients and doctors looking to the CDC for guidance in decision-making receive low quality or dated information. The mainstream media is stuck between reporting public health dictates as valid, while being unable to resist doom-and-gloom reports of vaccine “failures” that sell ad space. The obvious gap between “what the CDC says” and “what we see, hear and read” has left a large space for grifters, self-styled experts, and conspiracy theorists to thrive, especially among the large group of vaccine-hesitant (often vaccine-terrified) Americans. The whole thing might have gone better had we stuck to telling the truth as we knew it.
What follows is the truth about the Covid-19 vaccines, as I see it, from the data in hand right now. It is often inconvenient, especially for someone like me, who preferred the easy days of being a vaccine cheerleader when the initial trial data emerged. Do I still recommend a Covid-19 vaccine for the vast majority of my patients? Yes. It just takes a couple extra minutes to discuss now. Most importantly, if I speak the truth now, my patients will be more inclined to trust me later. So let’s see where we really stand:
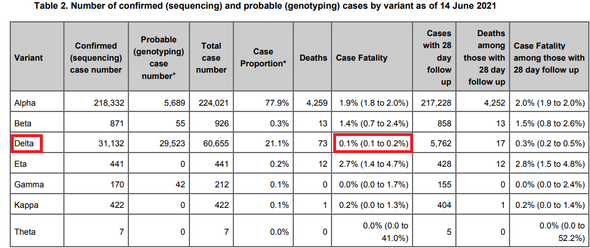
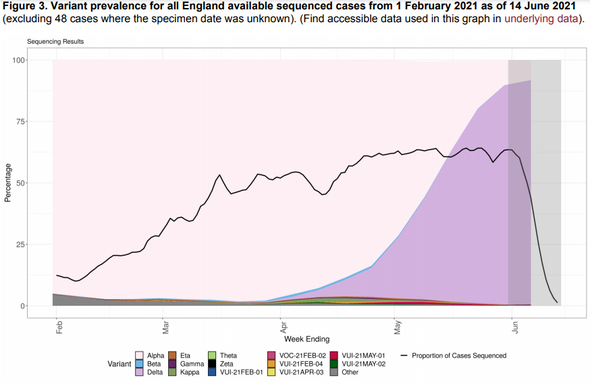
Let’s stop pretending the vaccines are 90% effective and breakthrough cases are “uncommon.”
The real world effectiveness of the Moderna and Pfizer (mRNA) vaccines appears to be sinking like a stone. We started at 94+% within 2 months of vaccination and against the original SARS-CoV-2 strain. The Israel Pfizer data roughly confirmed this degree of effectiveness in initial real world studies. But, then… waning happened, and delta happened. Pre-delta, we see that Pfizer final efficacy data from their trials dropped from 97% at two months to 84% by 5-6 months after full vaccination; Moderna, with its higher doses, dipped more modestly to 92%, although we might expect this number to fall soon enough, since Moderna tells us their neutralizing antibodies are sagging by the 6 month point. Unfortunately, the real world data is far more damning.
Right now, we have two widely-cited studies claiming 87-88% effectiveness for Pfizer against symptomatic infection: from Canada and the UK. Both studies, however, ended in May, in countries that spaced their two doses out by 2-3 months, leading to a short window after full vaccination.
What about studies of total infection rates (including asymptomatic infections, so we are a bit apples-to-oranges here) concluding in July in places with only a 3 week lag between Pfizer shots? Qatar: 56%. Mayo Clinic/US: 42%. Israel: 39%. Interestingly, the Qatar (85%) and Mayo (76%) data for Moderna were more positive, and time will tell us more about Moderna’s durability. It’s important to note that real world data is inherently messy – vaccinated people might just be different than their unvaccinated “case controls” in a study – but when the same pattern crops up with different investigators in multiple countries, it’s probably real.
Some of this is likely due to the delta variant’s modest ability to evade immunity. Neutralizing antibody responses among both those with prior infection and vaccination are several fold less to delta than the original SARS-2-CoV strain. However, I suspect the dramatic drop in effectiveness now being seen is a product of this immune evasion being amplified by waning immunity.
The truth here matters. For one, on a personal level, if you went from hiding in your house in March, to cheering on the local hockey team in June after your second Pfizer shot, it’s time to re-assess. Look at the recent UK REACT data: vaccinated people in mid-July were three times less likely than unvaccinated people to test positive for Covid-19. Great. But… they were almost twice as likely to test positive as unvaccinated people did just a month before, in mid-June! If you reduce your odds of infection by a factor of three with vaccination, but increase your risk of exposure by a factor of five, either due to rising prevalence or shifting your behaviors, you’re still more likely to catch a case of Covid-19 than if you had skipped the vaccine and stayed fixed in time. Put simply, regular high-risk exposures to SARS-CoV-2 can overwhelm a very good but imperfect vaccine.
Remarkably, the CDC is still proclaiming that vaccine breakthrough infections are rare – but when normal people hear that their barber, their cousin’s husband, and seemingly half the New York Yankees’ starters have experienced breakthrough infections, they might assume the CDC is lying.
Let’s stop pretending that vaccinated people are far less likely to spread SARS-CoV-2.
We have made pariahs of the unvaccinated as menaces to the public good. Even if this might not be the most effective form of public health messaging, perhaps this made statistical sense, at least, when we believed the mRNA vaccines to reduce all infections (including asymptomatic) by some 90%. Coupled with limited data from a UK study which showed household contacts of someone with a vaccine breakthrough infection were about half as likely to develop covid-19 as contacts of an unvaccinated person who became infected, it was reasonable to estimate that vaccinated people were almost 20 times less likely to transmit SARS-CoV-2 than unvaccinated people. This assumption led to the CDC’s recommendation that vaccinated people could drop their masks.
Unfortunately, the times, they are a-changing. The CDC famously reversed course on masks for the vaccinated. Data has been mixed, but several recent reports suggest the viral loads of those with vaccine breakthrough infections are akin to the unvaccinated. A thorough study from Singapore showed that vaccinated cases dropped their viral load faster — but viral loads were identical in days 1-5, when, logically, we might think most transmission takes place. Lacking a proper household transmission study post-delta, it’s simply not good science to assume the vaccinated spread less Covid-19 once they get infected.
From a societal perspective, is it reasonable to discriminate between the vaccinated and unvaccinated given this data? My second Pfizer shot was 7 months ago. An unvaccinated person without prior immunity is probably now only twice as likely to be infected as I am, but I can walk into a bar in New York City or Paris for a drink, and a VA hospital or Mayo Clinic for work — and they cannot.
Vaccine mandates and vaccine “passports” are often justified as necessary to reduce transmission of contagious diseases, but I don’t think the evidence is adequate at this point to make this claim for the Covid-19 vaccines. The substantial outbreaks in exceptionally well-vaccinated places like Israel, Malta and Vermont make it clear that pushing up vaccination rates does not guarantee control of Covid-19. Of course, the other justification for requiring Covid-19 vaccines is to limit the suffering and strain on society by reducing severe disease. Here, the legal and ethical questions are complex; and we must ask ourselves: is a potentially modest increase in vaccination rates worth the stress vaccine requirements entail?
Let’s stop pretending that it’s rare for vaccinated people to develop severe Covid-19 or die.
I cringe when I read Dr Anthony Fauci, CDC Director Rochelle Walensky, or Surgeon General Vivek Murthy remind us that 97% of new covid-19 hospitalizations or 99% of covid-19 deaths are among the unvaccinated. I know the message is well-intentioned: “Vaccines will protect you from severe disease, so go get vaccinated!” The problem is when the message is not quite true.
We saw this in the UK, where deaths among the vaccinated went from “rare” to two-thirds of all delta variant deaths by July. We saw this in Israel, where literally no fully vaccinated people died of covid-19 for entire weeks in June, but by August over 60% of the severely ill were fully vaccinated.
This is not evidence of vaccine failure; but those commentators who willfully misunderstand the base rate fallacy like to portray it as such. The reality is that Israel is so heavily vaccinated, especially among the elderly, that severe illnesses and death among the vaccinated will not be “rare” or even “uncommon” during a heavy, high-prevalence wave like they are having now. They will, however, be less common on a per capita basis than among the unvaccinated; about six times less common, as I write this.
Here in the US, there should be no shock value to reports of fully vaccinated people falling gravely ill with Covid-19. No vaccine is perfect, and half our population is fully vaccinated. However, many vaccine cheerleaders helped create an aura of perfection when it came to their touting of the vaccine trials: “Not a single death or hospitalization in the vaccine arms due to Covid-19 in over 75,000 participants!” Even without the arrival of delta and the recognition of waning immunity, no reasonable person would imply that there would be no deaths or hospitalizations once applied to 200 million participants.
From this expectation of bulletproof immunity, much of the public now feels betrayed.
Should they, though? When it comes to preventing severe infection or death, this is the great promise of the vaccines, and the clear basis for why I recommend them to almost all my patients. In all the studies I cited above with worrisome vaccine effectiveness against infection, virtually all still showed 90% or better effectiveness against hospitalization; the Mayo study was the outlier at 75%. So, to the best of our knowledge right now, if you get vaccinated you will be about 10 times less likely to be hospitalized with covid-19!
However, in the interest of truthfulness, there might be one substantial exception to that claim.
Let’s stop pretending that prior infection should not influence the decision to vaccinate.
Much has already been written about the CDC’s willful decision to ignore the relevance of prior infection, as if natural immunity simply did not exist. Most are aware that prior Covid-19 infection allows some degree of protection from future infection, with most studies suggesting this protection is north of 80% relative to someone with no immunity. It also leads to a greater immune response with first vaccination, which, in theory at least, could lead to better long-term protection, but also a higher rate of adverse effects. We are often told to “follow the science.” In this regard, there really is not much “science” to follow to endorse vaccination after infection.
Real world data is mixed; a recent study from Kentucky found two-fold additional protection to those with prior infection after full vaccination, while a larger study from the Cleveland Clinic showed no difference in re-infection rates between vaccinated and unvaccinated health care workers with prior infection.
Fortunately, we do have randomized controlled trial evidence to help shed light on the question. Unlike Johnson&Johnson, both Pfizer and Moderna tracked outcomes in their trials of those who had a history of Covid-19 infection before entering the placebo or vaccine arms. Moderna efficacy could not be evaluated due to having only one case in the placebo arm, while Pfizer showed a very modest 19% vaccine efficacy in the immunized group (vs 95% overall).
So – what does the science say? It says: barring new evidence, there is no clear benefit to immunizing those with confirmed prior infection. Common sense suggests there is a good chance these people would benefit from at least one (and possibly only one) shot as a “booster,” especially after 6 months or more have passed since the time of infection, especially with a more transmissible variant on the loose – but that’s common sense, not good quality data.
As a physician, I do think all but my lowest risk individuals with prior infection would have appreciable benefit from a single man-made “booster,” especially if they did not show evidence of antibodies, given the fairly robust correlation between a negative antibody test and risk of infection. However, I would not push if a previously infected patient opted to pass. As a citizen, I find it troubling that someone with prior infection could face an employer mandate to undergo vaccination against their will, given the slender evidence available.
Since we’re wading into divisive waters now, let’s dig into an even more charged subject: kids and vaccines.
Let’s stop pretending that the vaccines are a no-brainer for adolescents and children.
We parents are a sensitive bunch. Throw politics and heaps of fear-mongering into the equation, and talk of required vaccinations for school or sports quickly turns the volume up to 11. Lost in the noise, though, is that once again, evidence-based science is lacking that universal vaccination is appropriate for kids.
Virtually every American by now knows that Covid-19 severity drops with age. What no one knows is how well a Pfizer vaccine given to an adolescent today will reduce transmission by winter, and the adult data already discussed is concerning. So, are mostly left considering whether the risks of covid-19 to the lowest risk segment of our population outweigh the risks of the vaccine (and future boosters).
Just as no vaccine is perfectly effective, no vaccine is perfectly safe. The world has watched the adenovirus vector vaccines (AstraZeneca and Jansen/J&J) lead to serious thrombosis events mostly in younger women, and the mRNA vaccines trigger myocarditis mostly in younger men, roughly in the 1/10,000-20,000 range. To clarify: not 1%, not 0.1%, but <0.01%. These adverse reactions need to be acknowledged openly, however, as they are terrifying, and lead to chilling newspaper headlines and social media posts that make the possibility seem very real for your own child.
I explain the numbers to concerned parents like this: about 35 per 100,000 kids <18 in the US required hospitalization with Covid-19 in the first year of the pandemic. Even if half those hospitalizations truly were “with” and not “because of” Covid-19, that is still around 1 in 5-6000 of every American under 18. Could we be missing so much myocarditis, thrombosis, and whatever other vaccine-triggered illnesses are severe enough to lead to hospitalization, that the risk from vaccination could actually exceed the disease? It certainly seems unlikely, although that has not stopped some from twisting data to make this claim.
I also observe that these Covid-19 hospitalization rates are unlikely to stay this low, given the arrival of delta and it’s markedly higher transmission rates. What’s more, this calculation neglects the real concern for persistent disease from a covid-19 infection, aka “long covid,” which appears, very roughly, to affect somewhere in the 2-10% range of infected kids.
We must allow for some very small chance the mRNA vaccines will be the first vaccines in history to have a hidden adverse effect we missed in their first eight months of study. However, we must also allow for the chance that the virus itself might have some yet-unknown future harm, like the ability of Human Papilloma Virus and Epstein-Barr Virus to trigger certain cancers later in life.
All in all, I do think honest consideration of risk and benefit favors kids getting the Pfizer vaccine, and especially those with risk factors like obesity, asthma or diabetes, who make up the majority of hospitalized children. However, I think it’s important to remember that we are talking about 0.05%-type risks of serious disease versus 0.01%-type risks of severe vaccine reactions here – slim margins of benefit versus harm. I would rather the trial for the 12-15 year old age group had been larger than 1131 subjects in the vaccine arm to help us quantify those risks better.
A rational parent — especially the parent of a healthy boy, given the far higher rates of myocarditis in boys with the mRNA vaccines — could decide against giving their child the Pfizer vaccine, especially given the utter lack of certainty as to how soon and how often boosters will be required. Sensibly, I think, the UK took this approach: optional for those over 15, recommended for those 12-15 only with immunocompromised health status or high-risk family members, and gathering evidence for future decisions. My home state of Hawaii is taking rather the opposite approach, in mandating vaccination for all student-athletes. This is the unfortunate playbook for how to maximize vaccination in the lowest risk population group (athletes) half of whom are at the highest risk for requiring hospitalization for vaccine-mediated myocarditis (high school boys).
I don’t want to appear dismissive about the potential importance of vaccination for kids. While pediatric cases are rising and still roughly only half their prior peak levels from January, hospitalizations are already approaching that January peak, and we hear reports of pediatric ICUs filling, especially those under the strain of the current high rates of serious RSV cases. However, sometimes “do everything possible” is not the best long-game response to a short-term crisis. I question whether the reward of adolescent vaccination is so great and conclusively demonstrated that we should shame parents opting against this vaccine, or take schooling options away from their children.
Let’s stop pretending that a third booster is definitely going to help.
With recent approval for booster doses for the immunocompromised, they are today’s hot topic. While I am asked many questions about them, the truth is: I don’t have many answers. Pfizer has finally started a trial in in the past few weeks with 10,000 prior vaccine recipients. Once we get that data, perhaps in just a few months, we will move out of the theoretical realm.
Right now, theories are all we have. Perhaps one more dose of the original vaccine, by boosting overall antibodies, will help fight off the large infectious doses of delta. Or perhaps, by only stimulating the same imperfect antibodies, it won’t. Maybe the delta-specific boosters Pfizer and Moderna are developing will be ready for arms before the next variant arrives — and maybe not. Maybe we find new adverse effects with repeat doses of boosters. Maybe the extra protection lasts 4 months, or maybe years. Little is clear now.
Given their muted responses, on average, to their initial vaccine doses, the immunocompromised are most likely to benefit, and the most obvious candidates for a booster. Again though, this is based on laboratory studies of improved immune response, not actual trial data. As to the rest of us, I suspect the benefit will be modest, and/or quite possibly fleeting (remember, our annual flu shot’s efficacy fades about 10% per month, too). Until we see more definitive evidence that protection against severe disease truly is waning, I will be reluctant to recommend a booster except for my highest risk patients.
Let’s stop pretending that these vaccines are “kill-shots,” cause sterility, spread disease, etc.
Obviously, this is not directed at the public health community, but rather those who have built their social media brand by alarming the masses about the covid-19 vaccines. Everyone should have the right to raise their doubts and concerns about a new medical intervention. However, it is an abuse of that right to cherry-pick or deliberately misrepresent data while pretending to be impartial, or to sensationalize case reports without giving their context, with the sole purpose of breeding fear.
I try to read everything my patients and friends send me from these misinformers. They sprinkle into their missives bits and pieces of truth — generally the bits and pieces the CDC and WHO failed to mention — which lend them currency with their followers as “the only ones telling it like it is.” They don’t help their followers make rational decisions about vaccination, unfortunately.
Let’s stop pretending that the vaccines are the only way to reduce the burden of Covid-19.
No, I am not going to talk about Ivermectin here, having already said more than enough on the subject elsewhere. Our federal fascination with vaccination, however, has led to a frustrating lack of definitive research into potential treatments for covid-19, especially early in the disease course. We know HCQ failed; and that Regeneron’s monoclonal antibody treatments appear effective but are hard to access, costly and untested against delta; and that remdesivir only works a bit, and dexamethasone a bit more, but only for the very ill. Whatever happened to colchicine, famotidine, inhaled steroids, quercetin, fluvoxamine, and all the other potential agents which had an appealing study or two but never a large, definitive RCT? Perhaps a small diversion of some of the billions spent on vaccines could have led to an actual, evidence-based recommendation for physicians like me after our patients have a Covid-19 exposure or positive test. We literally have no CDC/NIH-endorsed treatments to offer that do not involve a trip to the hospital.
It’s also time to get real about obesity in this country. The US has an obesity rate of 36%, highest among “large” nations; for comparison sake, European nations generally fall in the 20-25% range, and Japan, South Korea, and China are all under 7%. At what point in the “pandemic era” does this become a national security risk? Studies of overweight/obesity on covid-19 hospital and ICU admissions suggest a 2- to 5-fold increased risk for the obese. That makes a normal BMI about a 65-85% effective “vaccine” against severe infection – one that keeps people out of the hospital from a variety of diseases, including the flu, and probably the next pandemic virus. Approaches to slimming down Americans come in many shapes and sizes, from Blue Zones concepts to soda taxes – which could be extended to all sweetened, calorie-dense processed and fast foods.
This pandemic has been an utter disaster. The next one might be worse. Bolstering our national capacity to fight off viruses would be a wise investment.
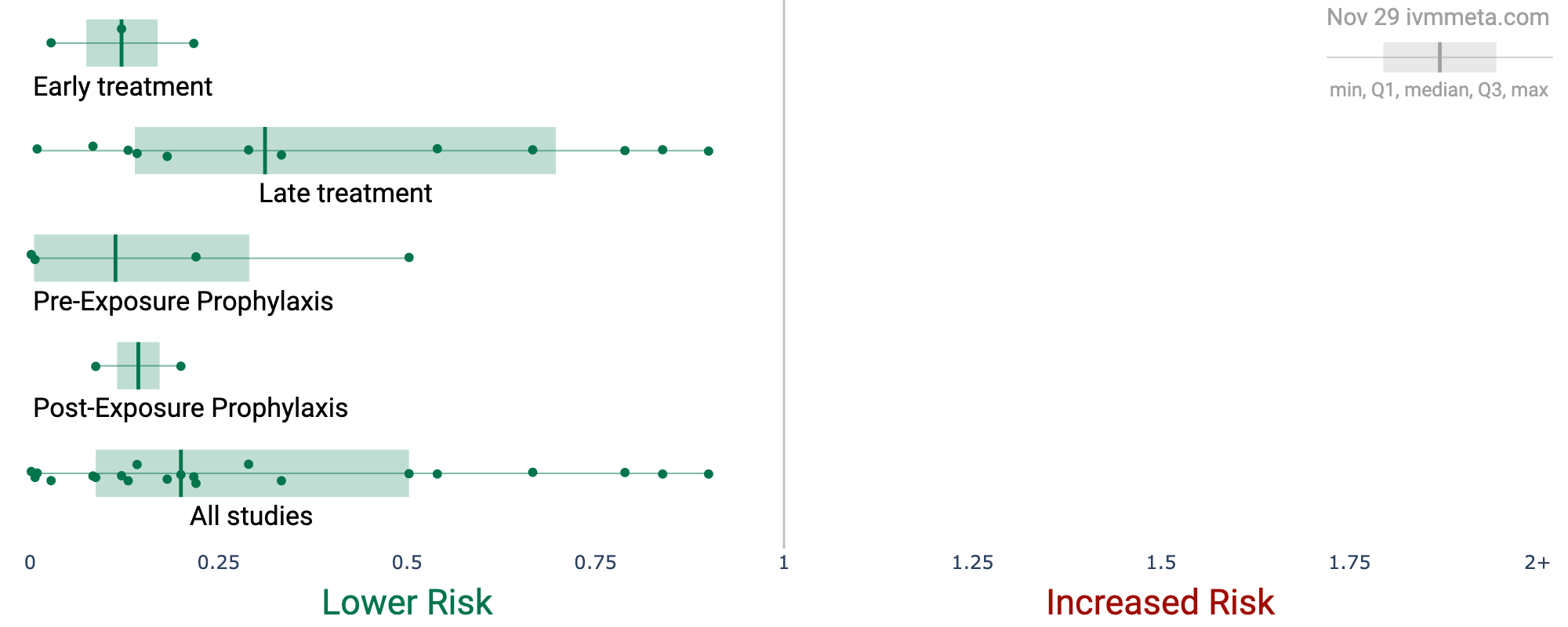
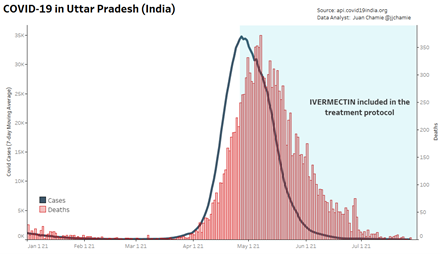
[My Comment: Hollander’s statement about HCQ is incomplete and thus misleading. “We know HCQ failed when given as a last resort to Covid patients on their death beds.” (There, Fixed.) No anti-viral works at that stage. Treatment with HCQ or Ivermectin is very effective early after infection to prevent a viral load able to cause severe illness. See Yes, HCQ Works Against Covid19 and Ivermectin Invictus: The Unsung Covid Victor Let’s stop pretending there are no effective early home treatments against Covid-19]
And, finally, let’s stop pretending that vaccines alone will bring an end to Covid-19.
Predictions have largely been useless in this pandemic. However, some basic principles are likely to hold true. We do not get to go back to alpha or the original strain of SARS-CoV-2; we are stuck with delta, likely until a variant even more transmissible mutates along and outcompetes it. That next variant will not have much evolutionary pressure to be either more or less severe; but imagining a variant able to spread even more rapidly than delta is dispiriting enough.
As more and more people gain immunity from infection and vaccination, there will be more pressure for SARS-CoV-2 to find its next host by evading immune defenses. It’s not hard to envision an eternal cat-and-mouse game in which reinfections are a commonplace event for all of us, and trying to avoid them will involve either a cycle of ever-shifting boosters, or acceptance that most 3rd, 4th or 5th SARS-CoV-2 infections will be mild enough to deal with.
The inconvenient truth is that neither natural immunity nor vaccines are likely to protect well enough, long enough, to shift this disease from pandemic to endemic and have it look the way most of us would prefer: partying like it’s 2019, and free of worry about hospital capacity. That, unfortunately, is probably a fantasy in the immediate future. So, too, is the idea that if we could only convince a few more stubborn vaccine hold-outs to get one set of shots that this will all be over and New Zealand can open its borders.
No, the way forward is going to be choppier than that. The “Covid long game” will involve uncertainty, surprises, and many hard choices, both for individuals and society as a whole. I hope we can be honest with ourselves as we make them.
Buzz Hollander MD is a family physician on the Big Island of Hawaii with no ideological axes to grind. He tweets @buzzhollandermd.
Protocols with HCQ or Ivermectin plus nutritional supplements fill the need for early home treatment