Only one question matters to people: What is my risk of getting Covid19 and dying from it? Daniel Horowitz explains that the Dutch have answered this question while the US CDC has not. See One chart exposes the lie behind universal lockdowns in the Conservative Review. Excerpts in italics with my bolds.
What is the true infection fatality rate of COVID-19, broken down by age and health status?
This is a simple question for which the CDC should have a clear answer by now, accompanied by a readable chart – a chart showing everyone’s demographic risk assessment so that we can better target our infection mitigation efforts.
Yet it’s the one thing our government hasn’t done. Wonder why?
Take a look at the above chart (which I translated into English using Google Translate) prepared by the Economisch Statistische Berichten (ESB), a Dutch economics magazine, quantifying the infection fatality rate for the Dutch population based on age bracket. The data were calculated from an antibody test of 4,000 blood donors conducted by Dutch blood bank Sanquin to see how many have been infected for the purpose of donating blood plasma to those currently suffering from the virus. The data were presented to the Dutch House of Representatives in mid-April by the National Institute for Public Health and the Environment (RIVM).
Based on this serology test, they were able to determine that 3% of the population (at the time) were infected and were therefore able to divide the numerator of those who died of COVID-19 by the extrapolated denominator of those who were likely infected and break out the infection fatality rate by age group.
Study this chart for a few minutes and take in all the data – from the asymptomatic/mildly symptomatic rates to the hospital and fatality rates divided by age. You have to get to the 50-59 age group just to reach a 0.1% fatality rate, the level often cited as the overall death rate for the seasonal flu. Those are all lower odds than an individual has of dying in a giving year of any cause and in the case of an average 50-year-old, five times lower.
They didn’t test kids under 20, but their fatality rate is likely near zero.
While the Netherlands is an entirely different country, it has actually experienced a 30% higher death rate per capita than America. So the numbers are likely not any higher here for those under 70, especially because the macro serology tests showing a 0.2% fatality rate (but grossly distorted by the death rate of those over 80), as well as what we are seeing in prisons and ships in younger populations, seems to harmonize with this data. A brand-new study from France also shows very similar estimates of fatality rates, at least for those under 60.
If anything, those who are sicker tend to stay away from blood donation, so it could be that infection rate was even higher than this sample suggests, thereby driving down the fatality rate even lower.
Moreover, several weeks later, another research group in the Netherlands did a second serology test that broke down even more groups and came up with almost identical results:
As you can see, the death rate doesn’t even climb above 1% until you reach over 70, with a steep and dangerous growth of risk over 75 and 80. However, it’s important to remember that even those death rates might need to be cut in half for those outside nursing homes, given that half the deaths in most countries are in senior care facilities.
Why has our government not put out a similar chart? How many Americans even know that children have near-zero threat and anyone under 60 has next to no risk of dying from the virus? Even those between 60 and 69 are at much lower risk than anything the government has suggested and that the level of panic indicates. The World Health Organization wrongly pegged the overall death rate for all ages at 3.4% on average. This simple fact makes a world of difference both to our targeted response to the virus and also to the degree of panic that should and should not be infused into society so as not to keep people away from hospitals when they are experiencing other potentially dangerous medical conditions.
But even this chart doesn’t tell the full story. The virus lopsidedly targets people with particular underlying conditions, such as heart disease and diabetes. It is simply criminal that, with the tens of billions of dollars in “emergency” funding, the CDC has not conducted or published the results of a survey of 20,000 or so Americans to determine the exact number of infections and the fatality rate broken down by each health and age status. To most Americans, based on what the government and media have been putting out, it’s all the same and even babies will all die, as if there is a 50% fatality rate. Most people I know think their infants are in danger from COVID-19, even though the threat of flu and SIDS is much more pervasive in infants than that of coronavirus.
Consequently, we destroyed our entire country and sacked the Constitution all for a very narrow and specific problem that required a precise and balanced approach. Yet two months into this mistake, our government won’t even put out the simple math demonstrating this obvious point. As one commentator so aptly observed,
“Homogenous intervention in the face of heterogenous risk is just cruelty passed off as equality.”
Those who have investigated global warming/climate change discovered that the numbers don’t add up. But if you don’t do the math you wouldn’t know that, because in the details is found the truth (the devilish contradictions to sweeping claims). Those without numerical literacy (including apparently most journalists) are at the mercy of the loudest advocates. Social policy then becomes a matter of going along with herd popularity. Shout out to AOC!
Now we get the additional revelation regarding pandemic math and the refusal to correct over-the-top predictions. It’s the same dynamic but accelerated by the more immediate failure of models to forecast contagious reality. Sean Trende writes at Real Clear Politics The Costly Failure to Update Sky-Is-Falling Predictions. Excerpts in italics with my bolds.
On March 6, Liz Specht, Ph.D., posted a thread on Twitter that immediately went viral. As of this writing, it has received over 100,000 likes and almost 41,000 retweets, and was republished at Stat News. It purported to “talk math” and reflected the views of “highly esteemed epidemiologists.” It insisted it was “not a hypothetical, fear-mongering, worst-case scenario,” and that, while the predictions it contained might be wrong, they would not be “orders of magnitude wrong.” It was also catastrophically incorrect.
The crux of Dr. Specht’s 35-tweet thread was that the rapid doubling of COVID-19 cases would lead to about 1 million cases by May 5, 4 million by May 11, and so forth. Under this scenario, with a 10% hospitalization rate, we would expect approximately 400,000 hospitalizations by mid-May, which would more than overwhelm the estimated 330,000 available hospital beds in the country. This would combine with a lack of protective equipment for health care workers and lead to them “dropping from the workforce for weeks at a time,” to shortages of saline drips and so forth. Half the world would be infected by the summer, and we were implicitly advised to buy dry goods and to prepare not to leave the house.
Interestingly, this thread was wrong not because we managed to bend the curve and stave off the apocalypse; for starters, Dr. Specht described the cancellation of large events and workplace closures as something that would shift things by only days or weeks.
Instead, this thread was wrong because it dramatically understated our knowledge of the way the virus worked; it fell prey to the problem, common among experts, of failing to address adequately the uncertainty surrounding its point estimates. It did so in two opposing ways. First, it dramatically understated the rate of spread. If serological tests are to be remotely believed, we likely hit the apocalyptic milestone of 2 million cases quite some time ago. Not in the United States, mind you, but in New York City, where 20% of residents showed positive COVID-19 antibodies on April 23. Fourteen percent of state residents showed antibodies, suggesting 2.5 million cases in the Empire State alone; since antibodies take a while to develop, this was likely the state of affairs in mid-April or earlier.
But in addition to being wrong about the rate of spread, the thread was also very wrong about the rate of hospitalization. While New York City found its hospital system stretched, it avoided catastrophic failure, despite having within its borders the entire number of cases predicted for the country as a whole, a month earlier than predicted. Other areas of the United States found themselves with empty hospital beds and unused emergency capacity.
One would think that, given the amount of attention this was given in mainstream sources, there would be some sort of revisiting of the prediction. Of course, nothing of the sort occurred.
This thread has been absolutely memory-holed, along with countless other threads and Medium articles from February and March. We might forgive such forays on sites like Twitter and Medium, but feeding frenzies from mainstream sources are also passed over without the media ever revisiting to see how things turned out.
Consider Florida. Gov. Ron DeSantis was castigated for failing to close the beaches during spring break, and critics suggested that the state might be the next New York. I’ve written about this at length elsewhere, but Florida’s new cases peaked in early April, at which point it was a middling state in terms of infections per capita. The virus hasn’t gone away, of course, but the five-day rolling average of daily cases in Florida is roughly where it was in late March, notwithstanding the fact that testing has increased substantially. Taking increased testing into account, the positive test rate has gradually declined since late March as well, falling from a peak of 11.8% on April 1 to a low of 3.6% on May 12.
Notwithstanding this, the Washington Post continues to press stories of public health officials begging state officials to close beaches (a more interesting angle at this point might be why these health officials were so wrong), while the New York Times noted a few days ago (misleadingly, and grossly so) that “Florida had a huge spike in cases around Miami after spring break revelry,” without providing the crucial context that the caseload mimicked increases in other states that did not play host to spring break. Again, perhaps the real story is that spring breakers passed COVID-19 among themselves and seeded it when they got home. I am sure some of this occurred, but it seems exceedingly unlikely that they would have spread it widely among themselves and not also spread it widely to bartenders, wait staff, hotel staff, and the like in Florida.
Florida was also one of the first states to experiment with reopening. Duval County (Jacksonville) reopened its beaches on April 19 to much national skepticism. Yet daily cases are lower today than they were they day that it reopened; there was a recent spike in cases associated with increased testing, but it is now receding.
Or consider Georgia, which one prominent national magazine claimed was engaging in “human sacrifice” by reopening. Yet, after nearly a month, a five-day average of Georgia’s daily cases looks like this:
What about Wisconsin, which was heavily criticized for holding in-person voting? It has had an increased caseload, but that is largely due to increased testing (up almost six-fold since early April) and an idiosyncratic outbreak in its meatpacking plants. The latter is tragic, but it is not related to the election; in fact, a Milwaukee Journal-Sentinel investigation failed to link any cases to the election; this has largely been ignored outside of conservative media sites such as National Review.
We could go on – after being panned for refusing to issue a stay-at-home order, South Dakota indeed suffered an outbreak (once again, in its meatpacking plants), but deaths there have consistently averaged less than three per day, to little fanfare – but the point is made. Some “feeding frenzies” have panned out, but many have failed to do so; rather than acknowledging this failure, the press typically moves on.
This is an unwelcome development, for a few reasons. First, not everyone follows this pandemic closely, and so a failure to follow up on how feeding frenzies end up means that many people likely don’t update their views as often as they should. You’d probably be forgiven if you suspected hundreds of cases and deaths followed the Wisconsin election.
Second, we obviously need to get policy right here, and to be sure, reporting bad news is important for producing informed public opinion. But reporting good news is equally as important. Third, there are dangers to forecasting with incredible certitude, especially with a virus that was detected less than six months ago. There really is a lot we still don’t know, and people should be reminded of this. Finally, among people who do remember things like this, a failure to acknowledge errors foments cynicism and further distrust of experts.
The damage done to this trust is dangerous, for at this time we desperately need quality expert opinions and news reporting that we can rely upon.
It did not take long after the onset of the global pandemic for people to observe the many parallels between the covid-19 pandemic and climate change. An invisible novel virus of the SARS family now represents an existential threat to humanity. As does CO2, a colourless trace gas constituting 0.04% of the atmosphere which allegedly serves as the control knob of climate change. Lockdowns are to the pandemic what decarbonization is to climate change. Indeed, lockdowns and decarbonization share much in common, from tourism and international travel to shopping and having a good time. It would seem that Greta Thunberg’s dreams have come true, and perhaps that is why CNN announced on Wednesday that it is featuring her on a coronavirus town-hall panel alongside health experts.
But, beyond being a soundbite and means of obtaining political cover, ‘following the science’ is neither straightforward nor consensual. The diversity of scientific views on covid-19 became quickly apparent in the dramatic flip-flop of the UK government. In the early stages of the spread in infection, Boris Johnson spoke of “herd immunity”, protecting the vulnerable and common sense (à la Sweden’s leading epidemiologist Professor Johan Giesecke) and rejected banning mass gatherings or imposing social distancing rules. Then, an unpublished bombshell March 16th report by Professor Neil Ferguson of Imperial College, London, warned of 510,000 deaths in the country if the country did not immediately adopt a suppression strategy. On March 23, the UK government reversed course and imposed one of Europe’s strictest lockdowns. For the US, the professor had predicted 2.2 million deaths absent similar government controls, and here too, Ferguson’s alarmism moved the federal government into lockdown mode.
Unlike climate change models that predict outcomes over a period of decades, however, it takes only days and weeks for epidemiological model forecasts to be falsified by data. Thus, by March 25th, Ferguson’s predicted half a million fatalities in the UK was adjusted downward to “unlikely to exceed 20,000”, a reduction by a factor of 25. This drastic reduction was credited to the UK’s lockdown which, however, was imposed only 2 days previously, before any social distancing measures could possibly have had enough time to work.
For those engaged in the fraught debates over climate change over the past few decades, the use of alarmist models to guide policy has been a familiar point of contention. Much as Ferguson’s model drove governments to impose Covid-19 lockdowns affecting nearly 3 billion people on the planet, Professor Michael Mann’s “hockey stick” model was used by the IPCC, mass media and politicians to push the man-made global warming (now called climate change) hysteria over the past two decades.
As politicians abdicate policy formulation to opaque expertise in highly specialized fields such as epidemiology or climate science, a process of groupthink emerges as scientists generate ‘significant’ results which reinforce confirmation bias, affirm the “scientific consensus” and marginalize sceptics.
Rather than allocating resources and efforts towards protecting the vulnerable old and infirm while allowing the rest of the population to carry on with their livelihoods with individuals taking responsibility for safe socializing, most governments have opted to experiment with top-down economy-crushing lockdowns. And rather than mitigating real environmental threats such as the use of traditional biomass for cooking indoors that is a major cause of mortality in the developing world or the trade in wild animals, the climate change establishment advocates decarbonisation (read de-industrialization) to save us from extreme scenarios of global warming.
Taking the wheels off of entire economies on the basis of wildly exaggerated models is not the way to go.
Footnote: Mark Hemingway sees how commonplace is the problem of uncorrected media falsity in his article When Did the Media Stop Running Corrections? Excerpts in italics with my bolds.
Vanity Fair quickly recast Sherman’s story without acknowledging its error: “This post has been updated to include a denial from Blackstone, and to reflect comments received after publication by Charles P. Herring, president of Herring Networks, OANN’s parent company.” In sum, Sherman based his piece on a premise that was wrong, and Vanity Fair merely acted as if all the story needed was a minor update.
Such post-publication “stealth editing” has become the norm. Last month, The New York Times published a story on the allegation that Joe Biden sexually assaulted a former Senate aide. After publication, the Times deleted the second half of this sentence: “The Times found no pattern of sexual misconduct by Mr. Biden, beyond the hugs, kisses and touching that women previously said made them uncomfortable.”
In an interview with Times media columnist Ben Smith, Times’ Executive Editor Dean Baquet admitted the sentence was altered at the request of Biden’s presidential campaign. However, if you go to the Times’ original story on the Biden allegations, there’s no note saying how the story was specifically altered or why.
It’s also impossible not to note how this failure to issue proper corrections and penchant for stealth editing goes hand-in-hand with the media’s ideological preferences.
In the end the media’s refusal to run corrections is a damnable practice for reasons that have nothing to do with Christianity. In an era when large majorities of the public routinely tell pollsters they don’t trust the media, you don’t have to be a Bible-thumper to see that admitting your mistakes promptly, being transparent about trying to correct them, and when appropriate, apologizing and asking for forgiveness – are good secular, professional ethics.
Study enrolling adults with mild to moderate COVID-19 in the United States.
A clinical trial has begun to evaluate whether the malaria drug hydroxychloroquine, given together with the antibiotic azithromycin, can prevent hospitalization and death from coronavirus disease 2019 (COVID-19). The National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, is sponsoring the trial, which is being conducted by the NIAID-funded AIDS Clinical Trials Group (ACTG). Teva Pharmaceuticals is donating medications for the study.
Transmission electron micrograph of SARS-CoV-2 virus particles, isolated from a patient. Image captured and color-enhanced at the NIAID Integrated Research Facility (IRF) in Fort Detrick, Maryland.NIAID
The Phase 2b trial will enroll approximately 2,000 adults at participating ACTG sites(link is external) across the United States. Study participants must have confirmed infection with SARS-CoV-2, the virus that causes COVID-19, and be experiencing fever, cough and/or shortness of breath. The investigators anticipate that many of those enrolled will be 60 years of age or older or have a comorbidity associated with developing serious complications from COVID-19, such as cardiovascular disease or diabetes. Participants will be randomly assigned to receive short-term treatment with either hydroxychloroquine and azithromycin or matching placebos. People living with HIV and pregnant and breastfeeding women also are eligible to participate in the study. The first participant enrolled today in San Diego, California.
“We urgently need a safe and effective treatment for COVID-19. Repurposing existing drugs is an attractive option because these medications have undergone extensive testing, allowing them to move quickly into clinical trials and accelerating their potential approval for COVID-19 treatment,” said NIAID Director Anthony S. Fauci, M.D. “Although there is anecdotal evidence that hydroxychloroquine and azithromycin may benefit people with COVID-19, we need solid data from a large randomized, controlled clinical trial to determine whether this experimental treatment is safe and can improve clinical outcomes.”
On March 28, FDA issued an Emergency Use Authorization (link) (EUA) to allow hydroxychloroquine and medical-grade chloroquine to be distributed from the Strategic National Stockpile and prescribed by doctors to hospitalized adolescents and adults with COVID-19, as appropriate, when a clinical trial is not available or feasible.
Participants in the ACTG study, called A5395, will receive oral medications to take at home. Those randomly assigned to the experimental treatment group will take 400 milligrams (mg) of hydroxychloroquine twice on the first day and 200 mg twice daily for an additional six days. They also will take 500 mg of azithromycin on the first day and 250 mg daily for an additional four days. The control group will receive equivalent numbers of placebo pills. Neither the participants nor the study team will know who received experimental treatment or placebo until the end of the trial.
Participants will record their symptoms, adherence to treatment, and major events such as hospitalizations in a diary for 20 days. Study staff will follow up with participants by telephone during this period. When possible, participants will come to the clinical research site for an in-person visit at day 20. Additional follow-ups will be conducted by telephone three and six months after treatment starts.
The main objective of the study is to determine whether hydroxychloroquine and azithromycin can prevent hospitalization and death due to COVID-19. Additionally, investigators will evaluate the safety and tolerability of the experimental treatment for people with SARS-CoV-2 infection.
“This study will provide key data to aid responses to the COVID-19 pandemic,” said ACTG Chair Judith Currier, M.D., of the University of California, Los Angeles. “We are pleased to be able to leverage ACTG’s existing infrastructure for HIV treatment clinical trials to quickly implement this important study.”
The study description at ClinicalTrials.gov is here. The program started May 1 and with a primary completion date of October 9, 2020.
Researchers at NYU Grossman School of Medicine looked at 932 coronavirus patients hospitalized between March 2 and April 5
Half were given a combination of hydroxychloroquine, azithromycin and zinc sulfate and the other half did not receive zinc
Patients receiving the triple drug combination were 1.5 times more likely to recover enough to be discharged and 44% less likely to die
The team believes hydroxychloroquine helps zinc, which has antiviral properties, get into infected cells
The main finding of this study is that after adjusting for the timing of zinc therapy, we found that the addition of zinc sulfate to hydroxychloroquine and azithromycin was found to associate with a decrease in mortality or transition to hospice among patients who did not require ICU level of care, but this association was not significant in patients who were treated in the ICU. This result may be reflective of the proposed mechanism of action of zinc sulfate in COVID-19. Zinc has been shown to reduce SARS-CoV RNA dependent RNA polymerase activity in vitro [13]. As such, zinc may have a role in preventing the virus from progressing to severe disease, but once the aberrant production of systemic immune mediators is initiated, known as the cytokine storm, the addition of zinc may no longer be effective [17]. Our findings suggest a potential therapeutic synergistic mechanism of zinc sulfate with hydroxychloroquine, if used early on in presentation with COVID-19. However, our findings do not suggest a prophylactic benefit of zinc sulfate in the absence of a zinc ionophore, despite interest in this therapy for prevention. A prophylactic strategy of zinc sulfate should be evaluated to help answer this question.
Background: Previous Post Preemptive Coronavirus Therapy
University of Minnesota is leading an important HCQ clinical trial, including collaboration with McGill University Montreal, University of Manitoba and University of Alberta. The initiative is called Post-exposure Prophylaxis / Preemptive Therapy for SARS-Coronavirus-2 (COVID-19 PEP) at ClinicalTrials.gov. Excerpts in italics with my bolds. H/T Don Monfort
Study Objective:
To test if post-exposure prophylaxis with hydroxychloroquine can prevent symptomatic COVID-19 disease after known exposure to the SARS-CoV-2 coronavirus.
To test if early preemptive hydroxychloroquine therapy can prevent disease progression in persons with known symptomatic COVID-19 disease, decreasing hospitalizations and symptom severity.
The Intervention Drug is Hydroxychloroquine. 200mg tablet; 800 mg orally once, followed in 6 to 8 hours by 600 mg, then 600mg once a day for 4 consecutive days Other Name: Plaquenil
On April 22, 2020, the independent Data and Safety Monitoring Board (DSMB) for the COVID-19 post-exposure prophylaxis trial has reviewed the cumulative safety data from 783 participants in the ongoing hydroxychloroquine prevention trial. The DSMB has identified no safety concerns or efficacy concerns at this time. We congratulate the study investigators on their enrollment thus far, and we will continue to provide oversight for the trial as specified in the DSMB charter.
Based on the event rate of COVID-19 illness observed in the control group, the sample size can be reduced by approximately one-third with approximately 200 more research participants needed to complete the trial to demonstrate conclusively whether or not there is a 50% reduction in symptomatic illness with a 5-day course of hydroxychloroquine after a high-risk exposure to someone with COIVD-19. The next interim analysis is scheduled for May 6, 2020. Ongoing U.S. enrollment is occurring at http://www.covidpep.umn.eduand in Canada at: http://www.covid-19research.ca
What Theory of the Disease Covid19 Suggests this Intervention?
In the United States and Europe, a handful of clinical trials have begun to test ways to keep healthcare workers and other vulnerable people safe from coronavirus disease (COVID-19).
Most are testing drugs called chloroquine or hydroxychloroquine that have long been used to prevent and treat malaria, and also as a therapy against rheumatoid arthritis and lupus. The hope is that, given before infection or early in the course of the disease, the drugs will protect someone against infection and illness from the virus, or, if they do, will ensure that their case is mild. But whether these drugs will help, hurt or do nothing remains an open question.
The virus that causes COVID-19 uses a backdoor to enter the cell. As it enters, it is exposed to an acidic, vinegar-like environment, which is actually needed for the virus to get all the way inside. Hydroxychloroquine, metaphorically keeps the cap on the vinegar, Greene says, preventing acidification. Thus, there is a scientific rationale for how this drug might exert an antiviral effect.
Mahir Ozmen, a professor of surgery at the Istinye University, School of Medicine in Istanbul, Turkey, says he thinks the best way to use chloroquine is in combination with zinc and vitamins C and D. He is running a clinical trial, testing to see whether this combination protects health care workers and their immediate families – including his own.
Ozmen, who is collaborating with a chest medicine specialist, an intensive care physician, and two infectious disease experts, says he intended to include only 80 participants, but 98 quickly volunteered. He began in April providing prophylactic therapy, and expects to complete the trial by July.
Ozmen says, “Hydroxychloroquine helps the zinc get inside the infected cells to destroy the virus, and vitamins A and D support immune function”. He gives volunteers a low dose of hydroxychloroquine every 3 weeks, and a vitamin tablet every day – or every other day for people prone to kidney stones. At the end of the trial, each participant will be checked for antibodies to COVID-19, suggesting an infection, whether they realised it or not.
This kind of prophylaxis will give us the time to develop a vaccine that will offer protection to everyone.
In perhaps the fastest-moving, large prophylaxis trial, researchers at Duke University are leading a US$ 50 million collaboration across hundreds of American healthcare systems, which will test 15,000 volunteers. Half the health care workers will take hydroxychloroquine, and half a placebo. Other drugs could be added to the study if they prove promising for preventing or lessening infection, says Adrian Hernandez, the trial’s principle investigator.
In France, researchers are running a trial with 1,200 healthcare workers to test prophylactic use of hydroxychloroquine or a combination of two HIV drugs, Lopinavir and Ritonavir, which failed as a treatment in people with severe COVID-19 infections but may work as prevention. It is expected to take 6 months.
In a 40,000-person trial led by the University of Oxford in England, participants in Asia will receive chloroquine or a placebo, and in Europe, hydroxychloroquine or a placebo. That trial is expected to take a year.
Footnote: A more detailed hypothesis for testing is provided by Dr. Scholz and Dr. Derwand of Leukocare in Munich (PDF here). Excerpt:
Based on the evidence of therapeutic effects of CQ/HCQ, their possible pharmacological effect as zinc ionophores and possibly underestimated specific and unspecific antiviral effects of zinc, we hypothesize that the combination of CQ/HCQ with parenteral zinc in the treatment of hospitalized COVID-19 patients may help to improve clinical outcomes and to limit the COVID-19 fatality rates.
Due to the existing substantial evidence, we propose to amend current clinical trial designs to test this hypothesis in the treatment of hospitalized COVID-19 patients by including at least one treatment arm with oral CQ or HCQ in combination with zinc. However, because of the better clinical safety profile HCQ should be preferred. To avoid interindividual differences of oral absorption rates and because of possible gastrointestinal side effects of oral zinc supplementation, it is proposed to use parenteral zinc preparations which are approved and clinically already used.
As the image above shows, supported by more detailed graphs below, Canada has now tested 1.17 million people with 6% positive for SARS-CoV-2 infection. 7% of those cases are reported deaths, or 0.45% of those tested.
The image presents coronavirus data as of the latest statistics complete to May 13, 2020. Note that Quebec accounts for 55% of all cases and deaths, most of them in Montreal, and mostly elderly residents in group homes. From the underlying data we can see that this Covid 19 outbreak started toward the end of the annual flu season. Since the graph is showing total accumulated cases, it can only go up until there are zero new ones.
To see the contagion in progress, here are the daily reported tests, cases, and deaths smoothed with 7 day averaging.
This outbreak is now about two months old. Note how cases early on rose along with the higher daily rates of testing, then held steady April 4 to 15 as testing declined slightly. Both testing and new cases then rose peaking on April 22 with 1806 new cases. Since then daily new cases have declined down to 1255 yesterday. Deaths per day peaked at 177 on May 5, and are down to 158 yesterday. (All daily figures are averages of the 7 day period ending with the stated date.) Tests went over 29,000 on May 9 and have continued at that level, about twice the daily number when April started.
The cumulative graph shows how the proportions faired during this period. Out of a total 1,172,872 tests, 72278 (6.2%) cases were detected, a rate down from 6.6% as recently as May 5. 5304 are reported deaths (7.3% of cases).
For context, below are the latest reported leading causes of deaths.
ln the last reported statistical year (2018) the top twelve causes resulted in 209,290 deaths, or 574 people dying every day. When we add in the less lethal killers, in 2018 in Canada, 283,706 people died, or 777 every day. This is not abnormal, but is the ongoing reality of our society where lives end for all kinds of reasons to make room for infants to be born and take their place among us.
Background from Previous Post
With coronavirus sucking all the air out of room globally, I got interested in looking at how the Canadian national flu seasons compare with the new Wuhan virus. The analysis is important since there are many nations at higher latitudes that are in equilibrium relative to infectious diseases, but vulnerable to outbreaks of new viruses. Where I live in Canada, we have winter outbreaks every year, but are protected by a combination of sanitary practices, health care system and annual vaccines, contributing to herd immunity.
For example, 2018-19 was slightly higher than a typical year, with this pattern: The various flu types are noted, all together making a total of 48,818 influenza detections during the 2018-19 season. A total of 946 hospitalizations were reported by CIRN-SOS sentinels that season (age = or >16). Source: Annual Influenza Reports
A total of 137 (14%) ICU admissions and 65 (7%) deaths were reported. The seasonality is obvious, as is the social resilience, when we have the antibodies in place.
For further background, look at the latest Respiratory Virus Report for week 13 ending March 28, 2020. [In this Respiratory Virus Report, the number of detections of coronavirus reflects only seasonal human coronaviruses, not the novel pandemic coronavirus (SARS-CoV2) that causes COVID-19. Kung Flu statistics are above at the beginning.]
For the period shown in the graph, 320560 flu tests were done, resulting in 32751 type A positives and 22683 type B positives. That is a ratio of 17% of tests confirming conventional flu infection cases. Public Health Canada went on to say in reporting March 22 to 28, 2020 (week 13): The percentage of tests positive for influenza fell below 5% this week. This suggests that Canada is nearing the end of the 2019-2020 influenza season at the national level. [Keep that 5% in mind]
Summary: It’s true that total cases and deaths are still rising, and everyone should practice sanitary behaviors and social distancing. But it appears that we are weathering this storm and have the resources to beat it. Let us hope for reasonable governance, Spring weather and a return to economic normalcy.
A provincewide clinical trial led by the University of Calgary will test the effectiveness of the anti-malarial drug hydroxychloroquine on COVID-19 patients, with the goal of reducing pressure on hospitals and preventing further infections.
“There is minimal evidence for use of hydroxychloroquine to use it, but there is enough (evidence) to study it,” said Metz, the acting facility medical director at Foothills Medical Centre and a professor in the department of clinical neurosciences at the Cumming School of Medicine.
“It just has to be done. If this drug does, indeed, reduce the severity and help people get better faster, it can help us in flattening the curve.”
The “HOPE” trial, to begin April 15, will target 1,600 Alberta outpatients who have tested positive for COVID-19 and are at risk of developing severe symptoms. The study will determine if hydroxychloroquine can prevent hospitalization for those at highest risk of developing a severe illness.
Participants will give their permission to Alberta Health Services after testing positive for COVID-19 and provide their contact information to U of C researchers. They’ll then be screened for safety and eligibility through a telephone interview and review of their electronic health record.
Those patients accepted will be sent hydroxychloroquine to their homes and will be required to take the drug over a five-day period. Researchers will follow up with participants seven and 30 days after starting the treatment.
Metz said timing of the trial is crucial and must begin within 96 hours of confirmation of a positive COVID-19 result, and within 12 days of symptom onset.
Should the drug prove effective, it may reduce the pressures that COVID-19 is expected to put on the health-care system.
“If we can keep more people out of hospital, then we’re not going to have that huge rise in hospitalizations and more people can get better at home,” she said. “Our system will get back to normal life or whatever we choose to move to in the future.
“We’ll be able to get there if we find this works.”
Hamilton Health Services starting an Anti-Covid19 study this month
The ACT COVID-19 program consists of two parallel trials evaluating azithromycin and chloroquine therapy (ACT) versus usual care in outpatients and inpatients who have tested positive for COVID-19. The trial is an open-label, parallel group, randomized controlled trial with an adaptive design. Adaptive design features include adaptive intervention arms and adaptive sample size based on new and emerging data.
Experimental: Azithromycin and Chloroquine Therapy (ACT)
Chloroquine (Adults with a bodyweight ≥ 50 kg: 500 mg twice daily for 7 days; Adults with a bodyweight < 50 kg: 500 mg twice daily on days 1 and 2, followed by 500 mg once daily for days 3-7), plus Azithromycin (500 mg on day 1 followed by 250 mg daily for 4 days) Source: ClinicalTrials.gov
With all the reporting on the pandemic, generalists are finding virology a steep learning curve, especially if one has been focused on climatology. A case in point: Recently the media reported on virus antibody testing of Major League Baseball (MLB) employees. Various headlines and stories drew differing conclusions about the import of the findings. Consider these few among many examples.
Inquiring scientific minds want to know if the large print is actually supported by what is stated in the small print. A fourth article in the Washington Postsuggested some of the places where digging for clarity is required. Excerpts in italics with my bolds
The study reportedly involved 26 of the 30 MLB teams and based its results on 5,603 completed tests and surveys. Researchers said 60 people tested positive for covid-19 antibodies, and after controlling for an expected amount of false positives and negatives, that number was adjusted to 42. There were zero deaths among the test group.
Researchers noted that the test group was not perfectly “representative of the American population at large,” because it skewed toward subjects who mostly ranged in age from 20 to 64 and who generally were of elevated socioeconomic status. [Note that this is a good sample of the work force, in contrast to all of the testing and cases involving elderly retirees from group homes.]
However, researchers pointed to the fact that the “overwhelming majority” of test subjects were not athletes but other types of team employees, from front-office executives to stadium vendors.
It takes about six to 10 days for 50 percent of people to develop antibodies, Bhattacharya said, and thus the snapshot provided by the study would have been from early April. MLB suspended spring training in mid-March, and it hopes to resume in June before starting to play games in July.
Bhattacharya said the 0.7 percent figure was surprising in part because players and team staffers would have been grouped together in spring training, in some cases in an environment featuring a higher than normal number of respiratory droplets, a few weeks before tests were completed April 14 and 15.
Bhattacharya said the study provided good news in the zero deaths but bad news by indicating that “the epidemic has not gotten very far.” Another positive takeaway could be gleaned from the fact that 70 percent of the subjects who tested positive described themselves as asymptomatic.
Like all viruses, SARS-CoV-2 needs to get inside human cells to multiply and survive. To do this, a particle on the outer shell of the virus latches onto a matching protein receptor, called ACE2, like a lock and key. ACE2 receptors are normally found in the lungs, kidneys, heart and the gut.
Once a person has been infected with the virus, it can take up to 14 days for symptoms to appear (if they do at all) – known as the incubation period.
The path from the point of infection can vary enormously. The body’s immune system is critical for determining this.
Having a strong immune response during the incubation period can prevent the infection taking hold, reduce the actual quantity of virus in the body and prevent it from getting to the lungs.
Some immune response basics
Our immune system offers us two lines of defence against viruses.
The first is the innate system and includes physical barriers such as skin and mucous membranes (the lining of the throat and nose), various proteins and molecules found in tissues, as well as some of the white blood cells that attack invading organisms. This immune response is general, non-specific and kicks in quickly.
Children have immature immune systems, but one hypothesis to explain why they don’t seem to get as sick with COVID-19 is that their innate immune response to coronavirus is greater than in adults.
This may lead to a reduced viral load – the quantity of virus particles that survive in the body – because they’re able to clear the virus more quickly.
The second line of defence is the adaptive immune response. This takes longer to initiate but once established, is much more efficient at eradicating a specific infection when encountering it again.
It’s thought that very specific genetic variations in some people might play a part in how sick they get. By generating an early adaptive immune response, the body seems to recognise the virus during the incubation period and fight it off.
A person also needs to be generally healthy to be able to mount an appropriate immune response to the infection.
After the incubation period, what determines how sick you get?
If the SARS-CoV-2 virus survives beyond the point of entry to the body (nose, eyes, throat) it might then make its way down the respiratory tract into the lungs.
In the lungs, it latches onto ACE2 receptors and continues replicating itself, triggering further immune responses to clean out infected cells. The amount of virus that gets deep into the lungs may be another important factor determining how sick you get.
As the battle between virus and immune responses proceeds, infected airway linings produce large amounts of fluid that fill the air sacs, leaving less room for transferring oxygen into the bloodstream and removing carbon dioxide. Symptoms of pneumonia appear, such as fever, cough with sputum (phlegm) and shortness of breath.
For some people, the immune response is excessive or prolonged and causes what’s known as a “cytokine storm”. Cytokines are a group of proteins that send signals to cells in the immune system, helping direct the response. A cytokine storm is a catastrophic overreaction that causes so much inflammation and organ damage, it can be fatal.
In people with COVID-19, as well as the previous SARS and MERS coronaviruses, this causes acute respiratory distress syndrome (ARDS), when fluid builds up in the lungs. This is the most common cause of death from SARS-CoV-2.
Elderly people and those with chronic lung disorders are more likely to develop ARDS and therefore to die. This is currently thought to be due to these groups of people having fewer ACE2 receptors in their lungs. This seems counter-intuitive, because the virus attaches itself to these receptors. However, ACE2 receptors have an important role in regulating the immune response, particularly in managing the degree of inflammation. So the reduced levels of ACE2 receptors in the elderly may actually make them more at risk of a cytokine storm and severe lung disease.
Conversely, children have more ACE2 receptors in their lungs which might explain why they do not get as sick.
In some cases, medications that work to suppress the immune system have successfully treated this excessive immune response in people with COVID-19.
Can people without symptoms pass it on?
Some studies have indicated people with COVID-19 tend to have a high viral load just before and shortly after they start getting symptoms. This suggests they can transmit it when they first get sick and up to 48 hours before, while they’re pre-symptomatic.
However, there is no good evidence that asymptomatic people who never develop symptoms are able to pass it on.
Researchers and clinicians are working around the clock to understand the complex relationship between humans’ immune systems and SARS-CoV-2 but it remains very much a work in progress.
Source: The Conversation Abela Mahimbo, Lecturer in Public Health, University of Technology Sydney; David Isaacs, Professor of Pediatric Infectious Diseases, University of Sydney; Melanie Wong, Head of Diagnostic Immunology Laboratory, Kids Research, and Melissa Kang, Associate professor, University of Technology Sydney.
An article at Clinical Chemistry discusses issues around the role of generic versus specfic coronavirus antibodies. SARS-CoV-2 Serology: Much Hype, Little Data. Excerpt in italics with my bolds.
What could be the reason for these false positive results?
Given the homology of SARS-CoV-2 to other coronaviruses, it is likely that antigens used as targets in poorly designed assays will cross react. This risk is exaggerated in older populations who are likely to have been exposed to a wider variety of coronaviruses (12). Many serologic assays also cross-react in patients with EBV, rheumatoid factor, and heterophile antibodies. Careful antigen selection in COVID-19 serological assays is required to avoid cross reactivity of anti-seasonal coronavirus antibodies. If validation studies are not designed appropriately (ie. if only young, asymptomatic pre-pandemic patients are used as the negative population), then these limitations may not be thoroughly vetted and specificity of the assay may be grossly overestimated. [Note the authors are concerned with overestimating cases with SARS CoV-2 specific antibodies by counting presence of other coronavirus antibodies. They do not consider the possibility that other generic antibodies act against SARS CoV-2 infection.]
It’s months into the coronavirus pandemic and public health officials still don’t know how many people have actually contracted the culprit, SARS-CoV-2. In many countries testing capacity has lagged behind the spread of the virus. Large numbers of people have developed COVID-19symptoms but have not been tested, and the vast majority of people who had the virus but never developed symptoms and therefore were not tested, are not reflected in official statistics.
Federal and state governments, companies, and research groups are now racing to develop antibody tests to shine a light on the true spread of SARS-CoV-2. While PCR tests currently used to diagnose cases detect the virus’s genetic material, antibody tests can screen for virus-attacking antibodies that are formed shortly after an initial infection. Those antibodies usually linger in the blood long after the virus is gone. One such antibody, or serological, test was given emergency use authorization by the Food and Drug Administration in early April, and a number of other groups are making more tests, and in some cases even deploying them.
The National Institutes of Health has launched a study to detect antibodies in order to gather data for epidemiological models. And a recent survey of residents in a German town was one of the first to use an antibody test among the public, reporting that 14 percent of people there were likely to have been infected with SARS-CoV-2 due to the presence of antibodies.
It’s not clear yet whether milder or asymptomatic cases will develop antibodies.
Policymakers have another reason to scramble to deploy antibody tests: they could indicate whether someone is immune to SARS-CoV-2. With around 3 billion people globally under lockdown, pressure is mounting to re-open national economies. In recent weeks, several politicians have proposed the idea of “immunity passports” or “immunity certificates” to identify people who have had the virus and therefore gained immunity to it and could re-enter the workforce again. Officials in Germany, the UK, Italy, and the US are already discussing such proposals.
The success of such a program hinges on:
whether everyone who has contracted SARS-CoV-2 actually develops antibodies,
whether those antibodies protect against secondary infections, and if so,
how long the antibodies hang around in the body.
So far, scientists don’t have firm answers to any of these questions. Although antibody surveys of communities around the world could yield information that is crucial to understanding the spread of the pathogen, some consider the idea of “immunity passports” premature.
“People understand that [it] would be very powerful, if we could say, ‘you’re immune now, and you can return to work,’ or, ‘you could safely return to your family if you’re a healthcare worker,’” notes Stanford University and Chan Zuckerberg Biohub immunologist Taia Wang. But there are a lot of unknowns, she cautions. “To get to that point where we’ll know with some certainty what the antibody response means, we just have to collect [more] data.”
The antibody response to SARS-CoV-2
There is solid evidence emerging that COVID-19 patients are developing antibodies to the virus, as the human body does for most infectious pathogens. Kara Lynch, a clinical chemist at the University of California, San Francisco, and her colleagues have been testing around 500 serum samples from roughly 100 COVID-19 patients who were treated at the Zuckerberg San Francisco General Hospital, where Lynch co-directs a clinical chemistry laboratory. The team is using an assay that was applied to samples from patients in China and picks out antibodies that target a protein-binding site of the virus’s spike protein.
“What we’re seeing is that patients are [developing antibodies] anywhere from two to about fifteen days” after developing symptoms, Lynch says. In most patients, the antibody response is broadly reminiscent of the typical reaction to many other pathogens: first, a flush of IgM, a generic type of antibody, followed later by the longer-lasting and more-specific IgG antibodies. Other studies have yielded similar results and suggest that antibodies circulate in the blood of COVID-19 patients for at least two weeks.
The data are skewed toward severe cases, however, as most of the subjects that Lynch’s group tested had been hospitalized, and it’s not clear yet whether milder or asymptomatic cases will develop antibodies, Lynch notes. “I’m optimistic [but] I’m still a little bit cautious.”
Recently, researchers at Fudan University in Shanghai examined the plasma from 175 COVID-19 patients who recovered after mild symptoms. The vast majority of patients developed antibodies that targeted the spike protein around 10 to 15 days after symptom onset, the scientists reported in preprint. The report generated some concern on social media because the researchers couldn’t detect antibodies in 10 of the patients. That could have been a fluke, notes Shane Crotty, an immunologist at the La Jolla Institute for Immunology. It’s possible that that the PCR test for SARS-CoV-2 was a false positive, and those people in fact had a different respiratory infection.
It’s also possible that some patients simply don’t develop antibodies.
While years ago, “pretty much everybody infected with SARS made an antibody response,” Crotty says, that did not hold true for MERS. Some studies on MERS have found that PCR-positive mild or asymptomatic infections can cause varied immune responses that are undetectable in antibody assays. Lynch points out that in her cohort, there are three patients who have not yet developed antibodies even though it’s been 17 days or more since their symptoms started. Some of those patients were immunocompromised, “but there are examples of healthy individuals that did not generate antibodies,” she writes in an email to The Scientist.
In many viral infections, “the magnitude of an antibody response correlates well with how big the infection was,” Crotty notes. In other words, severe infections are more memorable to the immune system. Interestingly, the preprint on COVID-19 patients in China also reported a positive correlation between the patients’ antibody levels and their age, which in turn, is known to correlate with the severity of COVID-19 symptoms. If it were the case that milder SARS-CoV-2 infections are less likely to produce a detectable antibody response, that may reduce the usefulness of antibody tests in detecting asymptomatic or mild cases.
Are the antibodies actually protective?
Overall, Crotty says he finds the data from the Chinese study robust and encouraging, noting that the researchers had extracted the patients’ antibodies and conducted in vitro experiments to see if they prevented SARS-CoV-2 from entering human host cells. “They tested 175 people and almost all of them had really nice antibody responses and really nice neutralizing responses,” he says. This is consistent with a recent study in macaques, and some other studies that have extracted antibodies from COVID-19 survivors and also found those antibodies were neutralizing, that is, capable of binding to the virus and its blocking entry into host cells.
Those experiments are important, and the results encouraging, but it’s still a mystery whether neutralizing activity in vitro correlates with protection in vivo for SARS-CoV-2, Wang notes. And even if antibodies aren’t neutralizing—and don’t physically stop the virus from entering host cells—they can still play important roles in immunity by recruiting other components of the immune system. “In vivo, there are many more cells that come into play to clear virus, to clear infected cells,” says Wang. It may well be that other components of the immune system—such as helper T cells or killer T cells—also play important roles in protecting against SARS-CoV-2.
On the whole, Wang finds it too early to say what the role of antibodies is for SARS-CoV-2. “We have no idea if production of antibodies during a primary infection, for example, has any role in clearing virus during that infection, or for that matter, we don’t have any good data on whether antibodies produced during an infection are protective against a second infection,” she says. And even if they were protective, they may not be protective for everyone. “Antibody responses can vary tremendously from person to person.”
How long will antibody levels last?
Ideally, the human antibody response to SARS-CoV-2 would mirror that to measles. A single exposure is enough to generate robust, neutralizing IgG antibodies that circulate in the blood throughout life and provide lifelong protection, Crotty notes.
But immune responses to coronaviruses appear to differ. Studies of survivors of the 2003 SARS epidemic suggest that concentrations of neutralizing antibodies lasted for up to three years. Although, a recent yet-to-be-peer-reviewed preprint reports to have found neutralizing antibodies in SARS survivors 17 years after the epidemic.
In MERS, the levels of neutralizing antibodies have been observed to fade after three years. For the less deadly, cold-causing coronaviruses, neutralizing antibody levels also fall off in that two-to-three-year range. One 1990 study of fewer than a dozen volunteers found that people exposed twice to the coronavirus 229E developed much milder symptoms compared with people getting exposed the first time, suggesting that re-infection could occur, but with reduced symptoms.
However, how long those cells or the antibodies they produce persist in the blood is not a surefast indicator of how long someone is immune to secondary infection, he stresses.
That’s because an initial encounter with a pathogen not only prompts the antibody-supplying cells, called plasmablasts, in the blood to turn into plasma cells that generate specific antibodies. It also stimulates memory B cells. These memory B cells can last decades, hiding out in lymph nodes, the spleen, bone marrow, and the lung, while some circulate in the blood. Upon re-infection by the same pathogen, they swing back into action, taking two-to-four days to differentiate into cells that secrete neutralizing antibodies, Menachery explains. He speculates that one might be able to acquire a second SARS-CoV-2 infection once the initial burst of neutralizing antibodies fades—which he reckons might be after one or two years—but the second infection will be milder thanks to immune memory.
It helps matters that SARS-CoV-2’s RNA genome appears to be relatively stable, meaning that the immune system may have a better chance of developing longer-lasting immunity compared to frequently-mutating influenza viruses, for instance, which require researchers to design new vaccines every year.
Summary: There are a lot of moving parts in this puzzle, and the observational record is short. The presence of SARS CoV-2 antibodies can estimate the minimum extent of people whose adaptive immune system fought off this virus. We are still in the dark about how many have been exposed to the virus but did not come down with the disease Covid-19 due to innate immunity.
Michael Schulson writes at Undark Magazine John Ioannidis Responds to Critics of His Study Finding That the Coronavirus Is Not as Deadly as Thought. Excerpts in italics with my bolds.
At issue here is a simple question: How many people actually have Covid-19? Ioannidis and other researchers from Stanford tried to answer that in a draft paper, or preprint, last month. Other experts began pointing out problems in the study, raising concerns about statistical errors, possible issues with a Covid-19 test kit, and shoddy sampling technique.
A few weeks later, the team released a revised version of the paper. The new draft, which, like the original version, has not yet received formal peer review, softens some of the more controversial claims, and acknowledges more uncertainty about the true number of infections.
The following interview — which covers the papers as well as Ioannidis’ appearances on partisan television — has been edited for length and clarity.
Undark: What kind of responses have you been getting so far to the revised draft?
John Ioannidis: Well, we’ve heard from several people. And I think that they’re happy that we have addressed the main issues that were raised on the first round. I also saw that [Columbia University statistician] Andrew Gelman, who was probably the most critical voice in the first round, has posted his appraisalof the revised version, which I think is very reasonable.
It’s hard to recall another paper that has been so extensively peer reviewed. [He laughs]. And lots of accounts were very useful and very constructive. The revised version has tried to address all the major concerns. I think the results are still very robust.
But it’s a single study. You can never say that a single study is the end of the story. You need to see all studies that are done, and by now there’s more than a dozen serology studies, and I think they pretty much paint the same picture.
UD: How so? In terms of estimates for how many infections there are, and what the infection fatality rate actually is — there still seem to be some substantial differences.
JI: Yeah, but this is entirely expected. Infection fatality rate is not like Avogadro’s number. It’s not a constant, like in a chemical experiment, the Km of an enzyme reaction. It’s affected both by how you count the [numerator] and how you count the denominator, and who are the people in the [numerator] and who are the people in the denominator. So, the case mix is very different in different locations. And the way that the serious cases were managed, or could be managed, is very different in different locations.k
So, depending on the setting and the population, the infection fatality rate may be from far less than influenza to far more — from the mild infection all the way to “This is disaster.”
D: I’ve seen your work being widely cited by people — including Fox News’ Tucker Carlson, who had you on as a guest — who are saying that the pandemic is not that serious, that it’s been overblown.
JI: I think that every citizen has the right to read science and try to make some sense of it. I cannot stop people’s interpretations of scientific findings, and it would not be appropriate for me to do that. So, yes, different people from different ideologies and from different backgrounds will read these results in different ways. But, this is not necessarily my reading or my interpretation. To be honest, as a scientist, I prefer to offer the data and try to be as calm as possible.
I think the main question is, should I or others, not talk to anyone — either Fox or CNN or BBC or Der Spiegel or Reuters or whatever? In principle, I have a problem with this perspective. It think that it creates a notion that scientists should not present the work. If you see some of these interviews — I mean, you mentioned Tucker Carlson, you can see my interview. And it’s obvious that I do not agree with lots of things that Tucker Carlson was proposing. At the same time, when he says that this virus is less lethal than we thought, this is accurate. It’s not who is saying it. It is whether this is an accurate statement or not. We started thinking that one out of 30 people will die. You know, when the [World Health Organization] made the announcement.
UD: Who thought that? The WHO said that 3.4 percent was the case fatality rate. Epidemiologists I’ve talked to said that it was clear the true infection fatality rate would likely end up being much lower. One scientist described the argument you’re making right now as “a straw man.”
JI: Well, let’s go back and check the exact announcement. [Note: The WHO announcement in question, from early March, specifies that “3.4 percent of reported cases have died.”] That was at the time when WHO had sent an envoy to China. And [the WHO envoy] came back and he said there’s no asymptomatic cases. Just go back and see what the statement was. He said there’s hardly any asymptomatic cases, it’s very serious and has a case fatality of 3.4 percent.
Of course, that [fatality rate] was gradually dialed back to 1 percent or 0.9 percent. And these are the numbers that went into calculations, and these are the numbers that are still in many of the calculations, you know, until very recently.
You know, 1 percent is, is probably like the disaster case, maybe in some places in Queens, for example, it may be 1 percent, because you have all that perfect storm of nursing homes, and nosocomial infection [an infection that originates in a hospital], and no hospital system functioning. In many other places, it’s much, much lower.
I’m trying to disentangle the accuracy of a scientific statement from who is making that scientific statement. Because if we don’t agree with who is making the scientific statement, then we run the risk of attacking the science, because it was just stated by that person.
We have to be very cautious here. I think that that’s going to be highly detrimental to science. My first opening statement in my first Fox interview was that science is the best thing that has happened to humans. I’m very proud to say that again and again and again.
Comment:
This is much the same as hysteria over global warming/climate change. All the hype is about tenths of a degree rise of an hypothetical number: Global Mean Temperature, which is estimated with multiple uncertainties, and hides great differences from place to place. And all the future damages are projected by computer models that assume GMT has a simple sensitivity to fluctuating amounts of CO2 in the atmosphere. The so-called climate crisis is the work of shamans not scientists, and Ioannidis is right to defend scientific integrity against such fear mongering.
And there is another similarity between climate and covid scares. Climatists obscure distinctions between weather and climate, between natural and human causation, and between the IR effects of H20 vs.CO2. Pandemic discussions typically blur or gloss over the difference between getting the virus and getting the disease. Just as having HIV (virus) is distinct from having AIDS (disease), so too it is increasingly clear a great many people are carrying SARS-CoV-2 (virus) without coming down with Covid19 (disease).
We know everything about Sars-CoV-2 and nothing about it. We can read every one of the (on average) 29,903 letters in its genome and know exactly how its 15 genes are transcribed into instructions to make which proteins. But we cannot figure out how it is spreading in enough detail to tell which parts of the lockdown of society are necessary and which are futile. Several months into the crisis we are still groping through a fog of ignorance and making mistakes. There is no such thing as ‘the science’.
This is not surprising or shameful; ignorance is the natural state of things. Every new disease is different and its epidemiology becomes clear only gradually and in retrospect. Is Covid-19 transmitted mainly by breath or by touching? Do children pass it on without getting sick? Why is it so much worse in Britain than Japan? Why are obese people especially at risk? How many people have had it? Are ventilators useless after all? Why is it not exploding in India and Africa? Will there be a second wave? We do not begin to have answers to these questions.
There is one vital fact that emerges from the fog. Countries that did a lot of testing from the start have fared much better than countries that did little testing. This is true not just of many Asian countries, such as South Korea (though Japan is an exception), but within Europe too. Up to the middle of last month, Iceland, Lithuania, Estonia and Germany had done many more tests per million people and recorded many fewer deaths per million people than Belgium, Britain, Italy and Sweden. As Max Roser of the website Our World In Data puts it: ‘The countries with the highest death rates got there by having the lowest testing rates.’
Yet it is not obvious why testing would make a difference, especially to the death rate. Testing does not cure the disease. Germany’s strange achievement of a consistently low case fatality rate seems baffling — until you think through where most early cases were found: in hospitals. By doing a lot more testing, countries like Germany might have partly kept the virus from spreading within the healthcare system. Germany, Japan and Hong Kong had different and more effective protocols in place from day one to prevent the virus spreading within care homes and hospitals.
The horrible truth is that it now looks like in many of the early cases, the disease was probably caught in hospitals and doctors’ surgeries.
That is where the virus kept returning, in the lungs of sick people, and that is where the next person often caught it, including plenty of healthcare workers. Many of these may not have realised they had it, or thought they had a mild cold. They then gave it to yet more elderly patients who were in hospital for other reasons, some of whom were sent back to care homes when the National Health Service made space on the wards for the expected wave of coronavirus patients.
The evidence from both Wuhan and Italy suggests that it was in healthcare settings, among the elderly and frail, that the epidemic was first amplified. But the Chinese authorities were then careful to quarantine those who tested positive in special facilities, keeping them away from the hospitals, and this may have been crucial. In Britain, the data shows that the vast majority of people in hospital with Covid-19 at every stage have been ‘inpatients newly diagnosed’; relatively few were ‘confirmed at the time of admission’. The assumption has been that most of the first group had been admitted on an earlier day with Covid symptoms. But maybe a lot of them had come to hospital with something else and then got the virus.
Even if you combine both groups, there are hardly enough admissions to explain the number of deaths in hospitals, unless nearly everybody admitted to hospital with Covid has died. It is likely that the frail and elderly, which the virus singles out for punishment, were more likely to be going to hospitals or clinics for other ailments and it was there that many of them got infected during February and March.
If Covid-19 is at least partly a ‘nosocomial’ (hospital-acquired) disease, then the pandemic might burn itself out quicker than expected.
The death rate here peaked on 8 April, just two weeks after lockdown began, which is surprisingly early given that it is usually at least four weeks after infection that people die if they die. But it makes sense if this was the fading of the initial, hospital–acquired wave. If you look at the per capita numbers for different countries in Europe, they all show a dampening of the rate of growth earlier than you would expect from the lockdowns.
This idea could be wrong, of course: as I keep saying, we just don’t know enough. But if it is right, it drives a coach and horses through the assumptions of the Imperial College model, on which policy decisions were hung. The famous ‘R’ (R0 at the start), or reproductive rate of the virus, could have been very high in hospitals and care homes, and much lower in the community. It makes no sense to talk of a single number for the whole of society. The simplistic Imperial College model, which spread around the world like a virus, should be buried. It is data, not modelling, that we need now.
If the elderly, obese and frail are not just at greater risk of dying, but also more susceptible and more infectious, then by definition everybody else is less so.
Gabriela Gomes and colleagues at the Liverpool School of Tropical Medicine looked at what would happen if the susceptibility of different segments of the population to the virus is very different, and concluded that in some circumstances effective herd immunity could be achieved with as little as 10 per cent of the population immunised. In the words of the study: ‘Individuals that are frailer, and therefore more susceptible or more exposed, have higher probabilities of being infected, depleting the susceptible subpopulation of those who are at higher risk of infection, and thus intensifying the deceleration in occurrence of new cases.’
If this is right, then it is good news. Once the epidemic is under control in hospitals and care homes, the disease might die out anyway, even without lockdown. In sharp contrast to the pattern among the elderly, children do not transmit the virus much if at all. This makes models based on flu, a disease that hits the young hard, misleading. The more the coronavirus has to use younger people to get around, the weaker its chances of surviving. Summer sunlight should slow it further, both by killing the virus directly and by boosting vitamin D levels.
It won’t be straightforward and there will be setbacks, but testing, followed by track and trace, is plainly now the way out. Britain is belatedly catching up. Matt Hancock’s ambitious dare to the healthcare system to get to 100,000 tests a day had the desired effect. We are now brimming with testing capacity, albeit still too centralised and slow in getting results back to people.
In the light of what we know, it is vital that the government now switches from urging us to stay at home to urging us to return to as much of normal life as possible. Be in no doubt that the strangulation that is asphyxiating the economy will have to be gradually lifted long before we know the full epidemiology of the virus.
Perilous though the path is, we cannot wait for the fog to lift before we start down the mountain.
Dr Deborah Cohen is an award-winning health journalist who has a doctor degree – which actually seems to be related to medical sciences – and who is working for the BBC Newsnight now. I think that the 13-minute-long segment above is an excellent piece of journalism.
It seems to me that she primarily sees that the “models” predicting half a million of dead Britons have spectacularly failed and it is something that an honest health journalist simply must be interested in. And she seems to be an achieved and award-winning journalist. Second, she seems to see through some of the “more internal” defects of bad medical (and not only medical) science. Her PhD almost certainly helps in that. Someone whose background is purely in humanities or the PR-or-communication gibberish simply shouldn’t be expected to be on par with a real PhD.
So she has talked to the folks at the “Oxford evidence-based medicine” institute and others who understand the defect of the “computer models” as the basis of science or policymaking. Unsurprisingly, she is more or less led to the conclusion that the lockdown (in the U.K.) was a mistake.
If your equation – or computer model – assumes that 5% of those who contract the virus die (i.e. the probability is 5% that they die in a week if they get the virus), then your predicted fatality count may be inflated by a factor of 25 assuming that the case fatality rate is 0.2% – and it is something comparable to that. It should be a common sense that if someone makes a factor-of-25 error in the choice of this parameter, his predictions may be wrong by a factor-of-25, too. It doesn’t matter if the computer program looks like SimCity with 66.666 million Britons represented by a piece of a giant RAM memory of a supercomputer. This brute force obviously cannot compensate for a fundamental ignorance or error in your choice of the fatality rate.
I would think that most 3-year-old kids get this simple point and maybe this opinion is right. Nevertheless, most adults seem to be completely braindead today and they don’t get this point. When they are told that something was calculated by a computer, they worship the predictions. They don’t ask “whether the program was based on a realistic or scientifically supported theory”. Just the brute power of the pile of silicon seems to amaze them.
So we always agreed e.g. with Richard Lindzen that an important part of the degeneration of the climate science was the drift away from the proper “theory” to “modeling”. A scientist may be more leaning towards doing experiments and finding facts and measuring parameters with her hands (and much of the experimental climate science remained OK, after all, Spencer and Christy are still measuring the temperature by satellites etc.); and a theorist for whom the brain is (even) more important than for the experimenter. Experimenters sort of continued to do their work. However, it’s mainly the “theorists” who hopelessly degenerated in the climate science, under the influence of toxic ideology, politics, and corruption.
The real problem is that proper theorists – those who actually understand the science – can solve basic equations on the top of their heads, and are aware of all the intricacies in the process of finding the right equations, equivalence and unequivalence of equations, universal behavior, statistical effects etc. – were replaced by “modelers” i.e. people who don’t really have a clue about science, who write a computer-game-like code, worship their silicon, and mindlessly promote what comes out of this computer game. It is a catastrophe for the field – and the same was obviously happening to “theoretical epidemiology”, too.
“Models” and “good theory” aren’t just orthogonal. The culture of “models” is actively antiscientific because it comes with the encouragement to mindlessly trust in what happens in computer games. This isn’t just “different and independent from” the genuine scientific method. It just directly contradicts the scientific method. In science, you just can’t ever mindlessly trust something just because expensive hardware was used or a high number of operations was made by the CPU. These things are really negative for the trustworthiness and expected accuracy of the science, not positive. In science, you want to make things as simple as possible (because the proliferation of moving parts increases the probability of glitches) but not simpler; and you want to solve a maximum fraction of the issues analytically, not numerically or by a “simulation”.
Science is a systematic framework to figure out which statements about Nature are correct and which are incorrect.
And according to quantum mechanics, the truth values of propositions must be probabilistic. Quantum mechanics only predicts the “similarity [of propositions] to the truth” which is the translation of the Czech word for probability (pravděpodobnost).
It is the truth values (or probabilities) that matter in science – the separation of statements to right and wrong ones (or likely and unlikely ones). Again, I think that I am saying something totally elementary, something that I understood before I was 3 and so did many of you. But it seems obvious that the people who need to ask whether Leo’s or Stephen’s pictures are “theories of everything” must totally misunderstand even this basic point – that science is about the truth, not just representation of objects.
PORTLAND, OR—Local man Trevor J. Gavyn pleaded with his conservative coworker to “believe the science on climate change,” though he himself does not believe the science on the number of genders there are, the fact that unborn babies are fully human, and that socialism has failed every time it has been tried.
“It’s just like, the science is settled, man,” he said in between puffs on his vape. “We just need to believe the scientists and listen to the experts here.”
“Facts don’t care about your feelings on the climate, bro,” he added, though he ignores the fact that there are only two biological genders. He also hand-waves away the science that an unborn baby is 100% biologically human the moment it is conceived and believes economics is a “conservative hoax foisted on us by the Illuminati and Ronald Reagan.”
“That whole thing is, like, a big conspiracy, man,” he said.
The conservative coworker, for his part, said he will trust the science on gender, unborn babies, and economics while simply offering “thoughts and prayers” for the climate.
On Monday, a reader, Max Anderson of Vancouver, wrote in to observe that, at this point in the COVID-19 epic, Canada does not appear to be doing so well by the developed world’s standards at preventing coronavirus deaths. The case isn’t complicated. It involves looking beyond the United States for comparisons, always a difficult optical exercise for Canadians.
Consider the OECD, the 37-member club of high-income liberal democracies. If you pull the COVID-19 death rates for these countries off of Wikipedia, you find a vast range of figures. Lucky Australia, as I write this, reports 4 fatalities per million residents; Japan and New Zealand are also at 4, with Slovakia and South Korea at 5. At the high end, Belgium, known to be liberal in its definition of a “COVID-19 death”, tops the table with 688 deaths per million. Spain is at 540, Italy at 483, and the U.K. in fourth place at 433.
But the median rate for the OECD countries is just 42 deaths per million, and Canada is at 99. So we probably shouldn’t feel smug because the U.S. stands at 209. Maybe we should be angry. Well, a lot of us are angry anyway.
A defence of Canada could start with the same data. A median is just the middle in a set of data points, the value at which half the things you measured are above and half below. The actual average, the mean, of OECD COVID-19 death rates is 128 per million. Suddenly Canada is doing better than average! A median and a mean can spread pretty far apart when a set of numbers isn’t symmetrically distributed, and in this case there are many small countries with death rates in the teens and 20s, including Latin American OECD members. (Those, with their rates, are Colombia, 7 per million; Chile, 14; and Mexico, 17.)
What’s astonishing here, I think, is the even-bigger-picture. Early in SARS-CoV-2’s bust-out from China, it became apparent that the heaviest impacts were in the very wealthiest countries. Eight or 10 weeks ago, there was widespread terror at the thought of what the virus would do when it reached the less developed world. This has, so far, proven to be the proverbial unbarking dog.
The website Our World in Data has a chart of countries with their per-capita GDP on the x-axis and their confirmed deaths per million on the y-axis. With logarithm scales on both axes, the data points on the chart are still, in May of the plague year, damned close to a straight line sloping upward from left to right. Allowing for differences in COVID case definition, there is, at the moment, no very poor country anywhere on Earth which has been hit significantly harder than Canada — and no large richer country that isn’t worse off aside from Norway.
Wealthy Canada is therefore more or less exactly where you would expect it to be on that chart (as is, for that matter, the U.S.A.). On the May 4 version of the chart we are in a little cluster, a mini-Pleiades, quite close to Germany, Austria and Denmark. Those are pretty comforting neighbours to have, I think (at least in this century). Denmark has perhaps the world’s best population-health data system. Germany is being celebrated for mobilizing the resources of the Robert Koch Institute, a federal disease control agency that can boast of actually controlling disease.
I think we can start believing, tentatively, that COVID-19 may be inherently a disease of affluence.
The assumption that it is only so circumstantially has prevailed for an awkwardly long moment. If GDP remains tightly correlated to national death tolls, countries are likely to judge themselves on whether they are high in the death table, or low, for their own particular degree of economic development.
It is not difficult to think of mediating factors that feed into the wealth-COVID relationship. Richer countries undertake more international business and pleasure travel, and attract more of it. The citizens within them are generally more mobile and more urbanized. People in the richer countries live longer, so their populations tend to have more old and vulnerable persons. Obesity is a known co-morbidity of COVID, and the rich countries have more of that, too — along with higher rates of hypertension and type 2 diabetes. And those countries are, of course, concentrated in one hemisphere of the globe: nobody knows anything meaningful yet about how weather (or any other regional phenomenon) affects SARS-CoV-2.
Add it all up and you get that (log-log) “straight-line” relationship. The trick, if the straight line continues to hold, will be sorting out exactly which correlates of GDP contribute, and how much. But the straight line is, in itself, quite surprising.
Anyone would have expected — and most experts still half-expect — that our lack of social deprivation, by itself, would more than compensate for lifestyle excesses and material privileges in a crisis like this. This is to say nothing of Canada’s sophisticated, and publicly provided, health-care system, which doesn’t seem to have bought us much extra protection against a nightmare from the past. No one expected an infectious disease with these special characteristics, which remain mysterious. We all joked around about “First World problems” for a long time. Anybody having a laugh at this one?
Footnote: Background on Modern Affluence
Alex Epstein (here) is among those who demonstrate from public information sources comparisons between societies who use carbon fuels extensively and those who do not. The contrast is remarkable: Societies with fossil fuels have citizens who are healthier, live longer, have higher standards of living, and enjoy cleaner air and drinking water, to boot. Not only do healthier, more mobile people create social wealth and prosperity, carbon-based energy is heavily taxed by every society that uses it. Those added government revenues go (at least some of it) into the social welfare of the citizenry. By almost any measure, carbon-based energy makes the difference between developed and underdeveloped populations.
In addition, developed societies protect most of their citizenry from natural disasters, including extreme weather events.
The EM-DAT database provides three disaster impact indicators for each disaster event: economic losses, the number of people affected and the number of people killed. . .The data show large differences across disaster indicators and regions: economic losses are largest in the OECD countries, the number of people affected is largest in the BRIICS countries and the number of people killed is largest in the RoW countries.
Fig. 3 Economic losses normalized for wealth (upper panel) and the number of people affected normalized for population size (lower panel). Sample period is 1980–2010. Solid lines are IRW trends for the corresponding data.
Clearly, the wealthier nations build and maintain more robust structures and infrastructures, which incur costly damages from natural events, but which greatly reduce human deprivation and deaths. Ironically, these advantaged nations now provide large numbers of attractive hosts for this novel coronavirus, absent defences from medical technology. It is also the case that these privileged populations are so rooted in presumed physical security that the hysterical media has triggered a panic pandemic, overshadowing the actual viral outbreak.
Postscript: For the latest social distancing etiquette as restaurants reopen:
Don’t try it you will die. This is a common misunderstanding of medical treatments. If I shoot your heart with Epinephrine during a heart attack it may save your life. It may even take a second shot or a third to work. But don’t even consider doing it a 4th time.
You see this is how that drug works. It causes the heart which in a heart attack is already dying for lack of energy to burn through its energy reserves even faster. The few doses work but by the 4th dose the heart has no reserve energy. You couldn’t get it to move if you tried.
All of the “good things” you think are happening with the COVID-19 lockdowns are exactly the same as with that heart. You are seeing a lockdown that appears to you to have no harm and the energy from outside is dropping so you think you have no problem. What you are not seeing is your society is fast burning through its vital resources. Very soon all the tricks will burn through all the resources and then NOTHING will work. Then people will be dying in masses from the treatment. If we get the world back to running as usual it make take a bit of “rehab” but we will get back and burn even more fuel to make up for the burned up reserves. It will take that to get us back to strong again.
What you are celebrating is DEATH happening! The reduction in fuel use must come from somewhere. Right now it is coming from the grain bins and from the prepackaged stores of energy that you call food. The nation states have commanded with lockdown and stimulus packages the exact situation with the heart and the epinephrine. They have told a dying economy to kick in the reserves. Stupid people think this can work for a long time. It cannot. It is fatal. You and your economy are being poisoned to try to cure a dangerous situation. Epinephrine is a deadly poison! Yes I do know the use of it very well I am ACLS and Heart Transplant qualified.
What is happening with the world’s ships parked and our cities shut down is that we are running out of energy. Oh yes the oil bins are full but the vital energy like fertilizer is not reaching the people in Africa etc. When they don’t get their stuff and their food and etc, the game will end very badly.
I think people arguing this have no idea what saved the whales from extinction. They think it was Greenpeace. It wasn’t. It was the discovery of Oil in Pennsylvania. You see the world was about to come to a halt from lack of whale oil and that was what drove the discovery. Oil saved the whales. You shut down the oil gas and coal and you will soon see all life swept from the land and the seas. You are not going to see a wonderful world, you are going to see a massive FAMINE!
Summary: Hunger and Poverty are the two greatest killers of humanity, and hundreds of millions of people are now at risk because of the global economic shutdown.
Scott Atlas explains the medical realities for ending the shutdowns now.




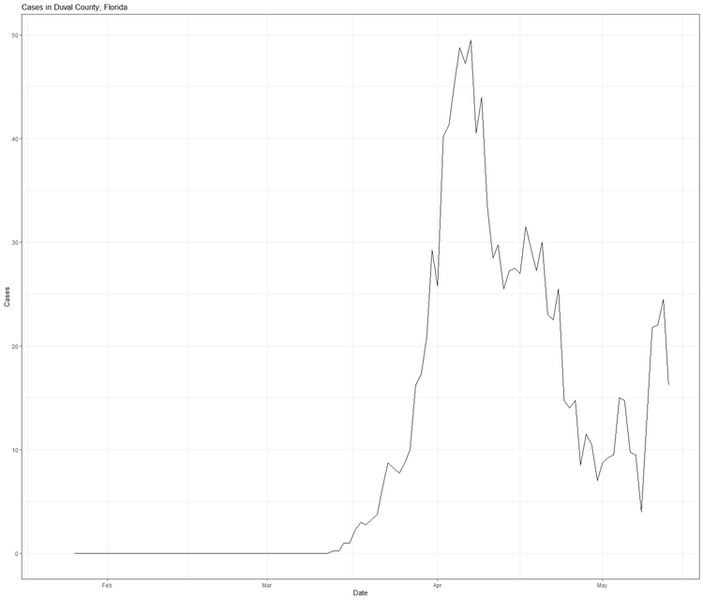
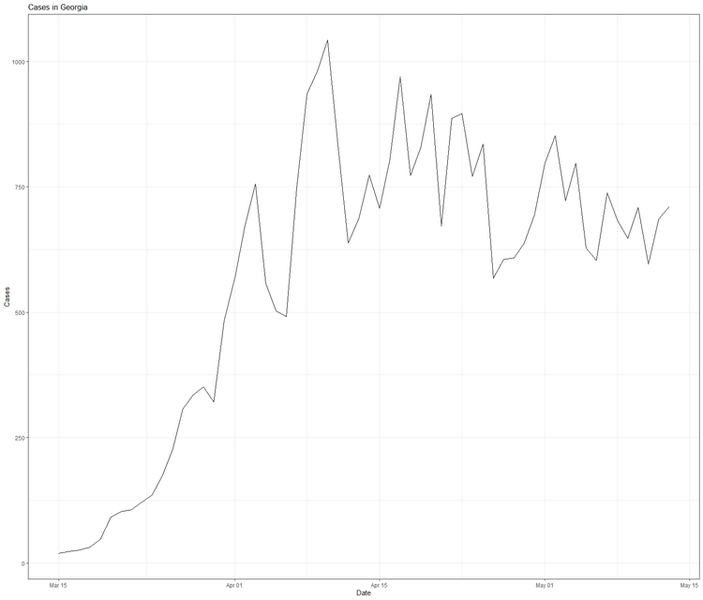


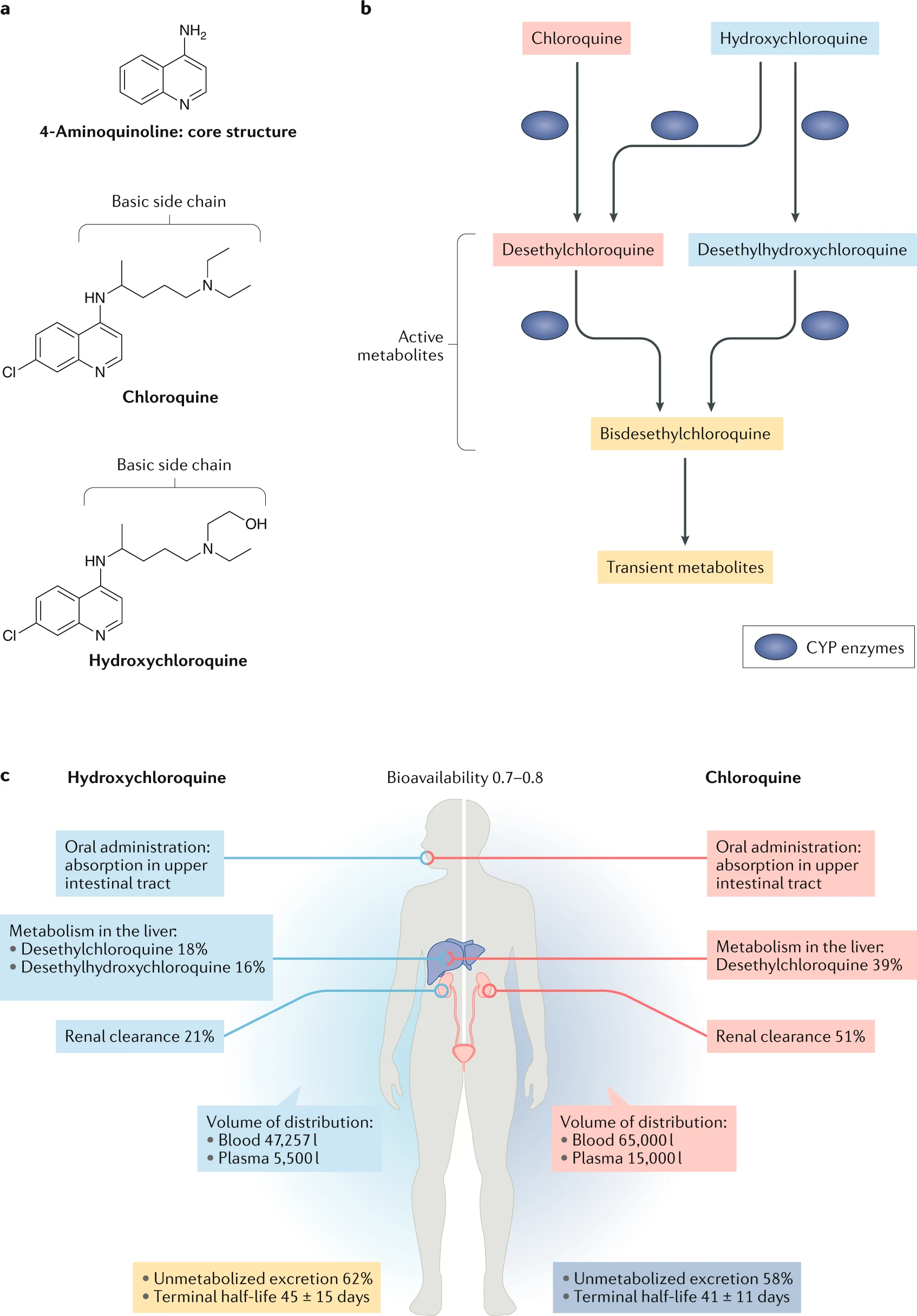
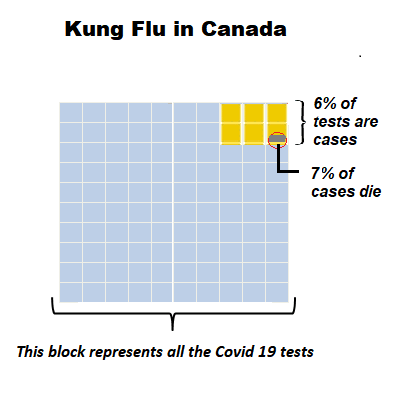
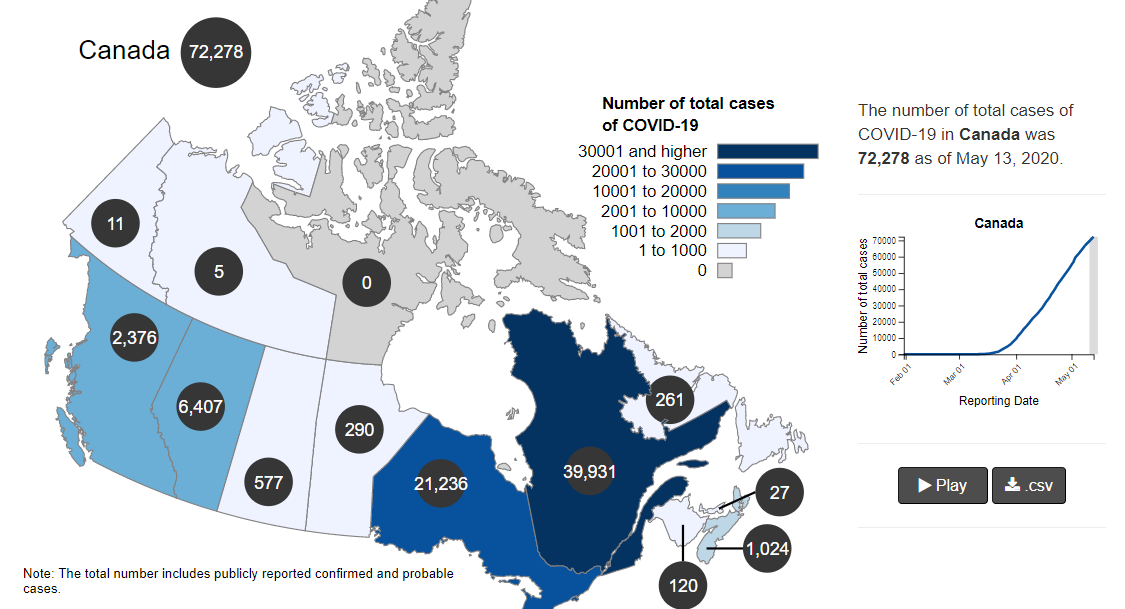
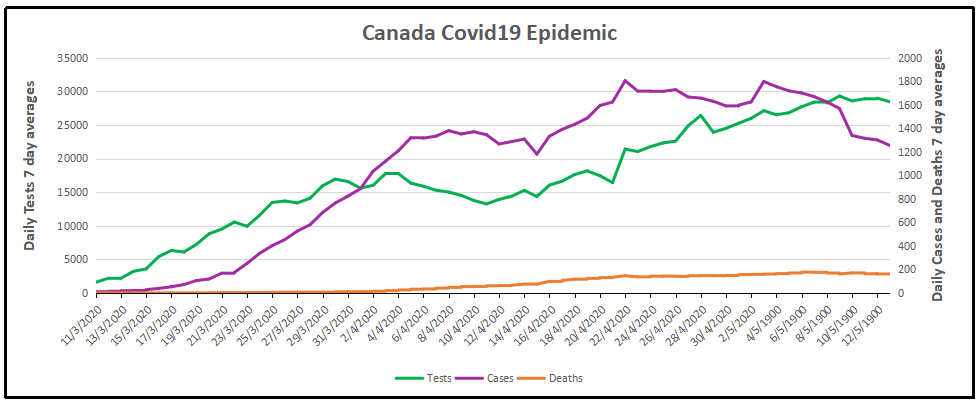
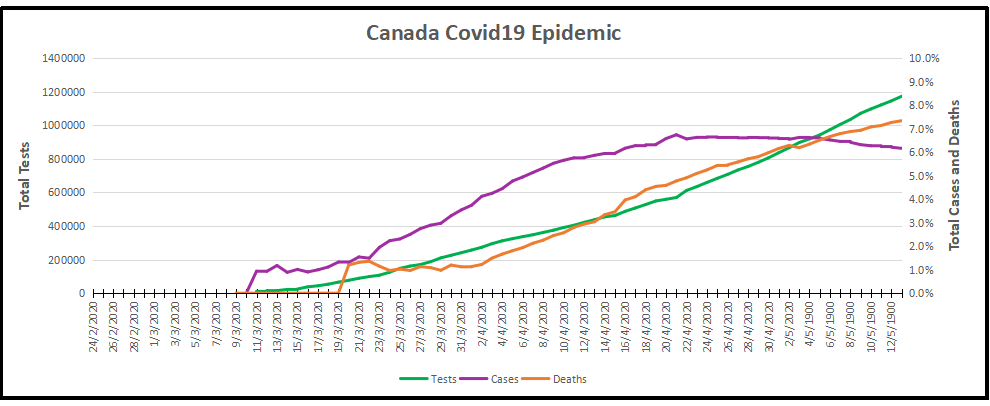

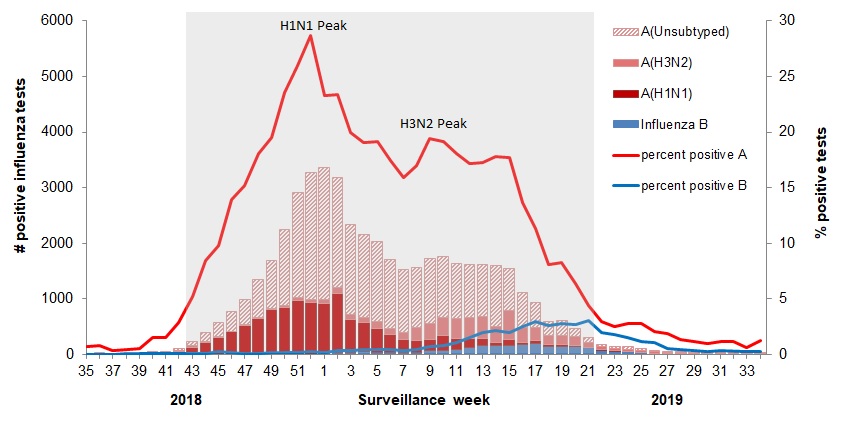 The various flu types are noted, all together making a total of 48,818 influenza detections during the 2018-19 season. A total of 946 hospitalizations were reported by CIRN-SOS sentinels that season (age = or >16). Source:
The various flu types are noted, all together making a total of 48,818 influenza detections during the 2018-19 season. A total of 946 hospitalizations were reported by CIRN-SOS sentinels that season (age = or >16). Source: 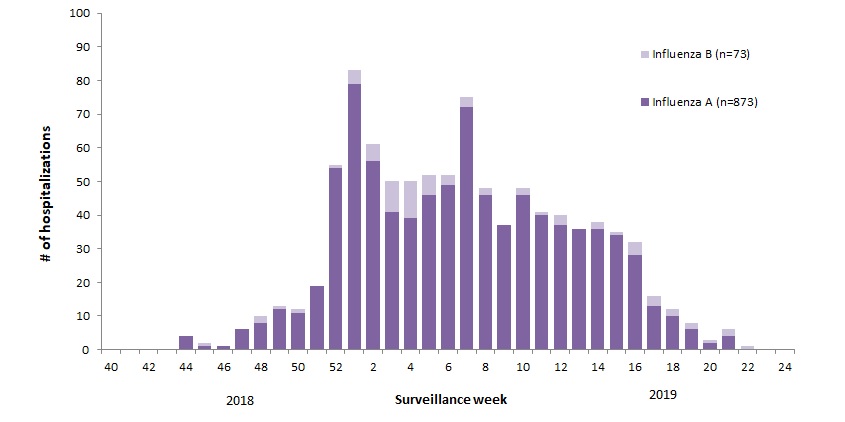
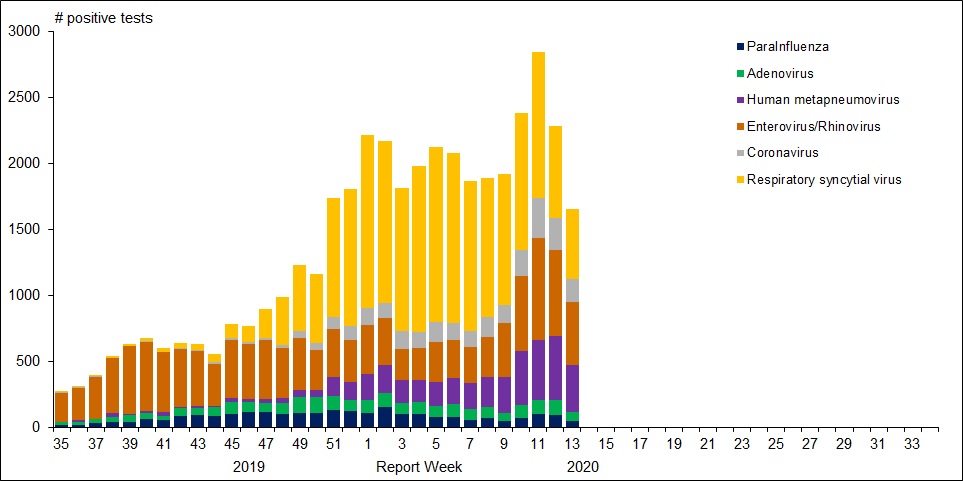




 Matt Ridley writes at the Spectator
Matt Ridley writes at the Spectator