Stanford Jumps Suicide Climate Shark

Today’s media feeding frenzy is promoting another scary climate change report from Stanford. Sample headlines are:
Climate change linked to increase in suicide rates USA Today
Rising heat linked to suicide spikes in U.S. and Mexico Thomson Reuters Foundation News
Climate Change May Cause 26,000 More U.S. Suicides by 2050 The Atlantic
Etc. Etc.
Some points to consider:
1. A suicide is a personal event with many contributing factors, weather and climate being the most peripheral.
2. Serious suicide researchers have identified risk factors that inform caregivers. Franklin et al. provide this analysis of experience with suicidal incidents Risk Factors for Suicidal Thoughts and Behaviors: A Meta-Analysis of 50 Years of Research
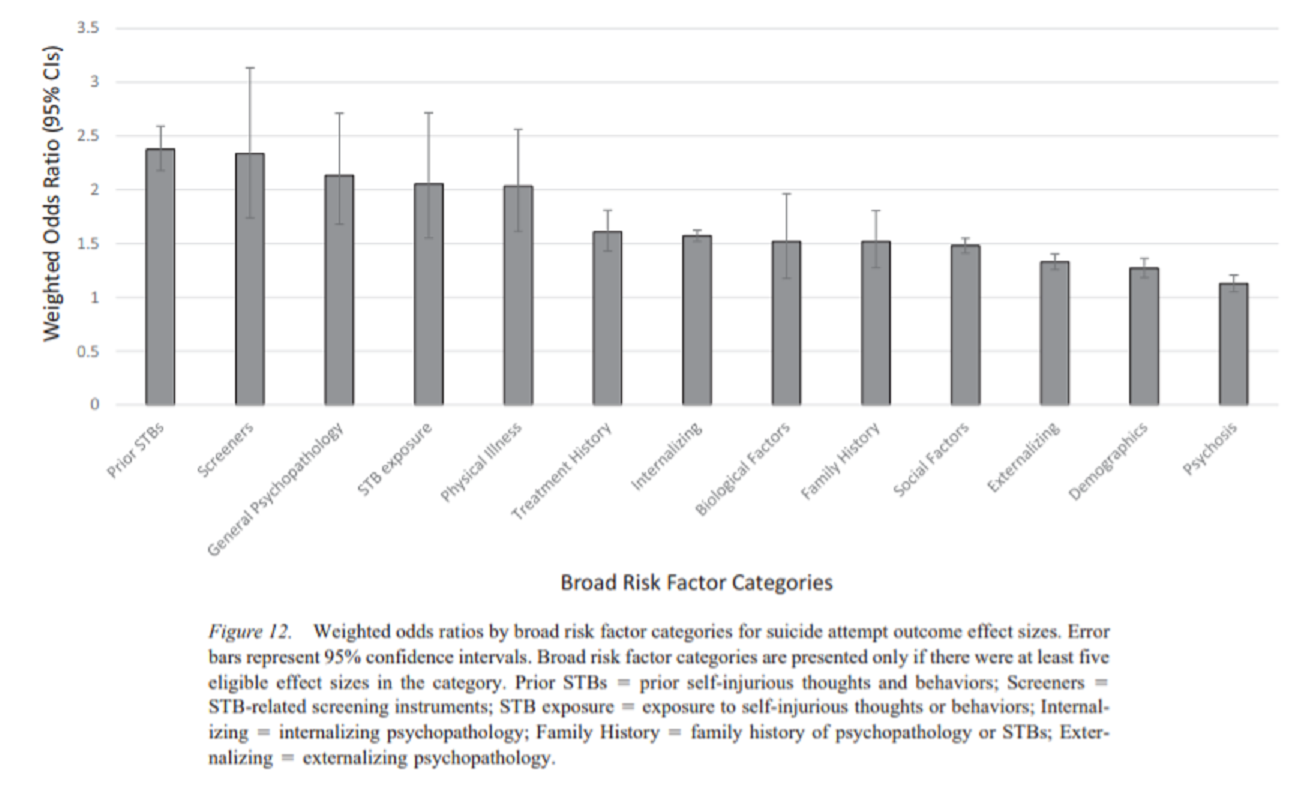
Open image in new tab to enlarge.
With such complexity of influencing factors, putting emphasis on a bit of warming is both myopic and lopsided. For example, some places report springtime suicides are more frequent, others see more such deaths in Summer or Autumn. The seasonal relationship is quite mixed in studies with various theories being suggested along with great uncertainty.
3. Suicides occur more frequently in colder climates than in warmer ones. For example, this European study found the highest rates in eastern European nations and lowest rates in Mediterranean countries.
Relationship of suicide rates with climate and economic variables in Europe during 2000–2012 in Annals of General Psychiatry. Excerpt below in italics with my bolds.
It is well known that suicidal rates vary considerably among European countries (Fig. 1) and the reasons for this are unknown although several theories have been proposed. The effect of climate has previously been discussed but has not been investigated in a systematic way across countries.
One of the biggest enigmas is the marked geographic variability in suicide rates found in Europe, with the highest rates being found in Eastern Europe and the lowest in the Mediterranean region
The current study reports that the climatic effect (cold climate) is stronger than the economic one, but both are present. It seems that in Europe suicidality follows the climate/temperature cline which interestingly is not from south to north but from south to north-east.
4. Preventing suicides is a serious issue, and has nothing to do with reducing CO2.
These New Zealand researchers argue against mixing climate policies with suicide prevention programs.
Will climate change increase or decrease suicide rates? The differing effects of geographical, seasonal, and irregular variation in temperature on suicide incidence Excerpts in italics with my bolds
The effect of environmental temperature on suicide risk is an important issue given the increase in global temperatures expected over the following century. Previous research has produced conflicting findings: Studies concerned with temporal variation in temperature and suicide have tended to find a positive relationship, while those concerned with geographical variation in temperature and suicide have tended to find a negative relationship. In this study, we aimed firstly to estimate the relationship between suicide incidence and three components of variation in temperature: Irregular, seasonal, and geographical. Secondly, we aimed to critically examine what this information can (and cannot) tell us about the likely effects of anthropogenic climate change on suicide rates.
In this study, irregular variation in temperature had a positive relationship with suicide incidence, with approximately 1.8% more suicides for every 1°C increase in temperature. The size of this estimate was fairly consistent with those of previous studies (e.g., Deisenhammer 2003; Kim et al. 2011). We did not find evidence of the non-linear relationship between temperature and suicide incidence reported by Page et al. (2007). We also found no evidence for any substantial lagged effect of irregular variation in temperature, a finding similar to that of Likhvar et al. (2011) and Kim et al. (2011).
On the basis of the apparent positive effect of irregular variation in temperature, it would be tempting to conclude that global warming will increase the incidence of suicides. However, this conclusion is contradicted by our analyses of seasonal and geographical variation in temperature and suicide. Seasonal variation in suicide deaths did roughly follow the pattern generally found in the literature of a peak in spring and a trough in winter (Chew and McCleary 1995), but in accordance with a previous study in New Zealand (Yip et al. 1998), the magnitude of seasonal variation in suicide incidence was very small.
Furthermore, seasonal variation in temperature had a relationship with suicide incidence that was close to zero: That is, hotter times of the year were not consistently associated with higher suicide risk The relationship between geographical variation in temperature and suicide incidence differed even more greatly from that of irregular variation in temperature. While there was little evidence of any relationship at a bivariate level, controlling for age and ethnic differences across regions resulted in the relationship becoming negative: warmer areas had lower suicide rates. This finding was in accordance with prior studies finding a negative relationship between geographical variation in temperature and suicide rates (Rotton 1986; Souêtre et al. 1990; Lester 1999).
Counteracting the potential confounding problem relating to analyses of seasonal and (especially) geographical variation is that these analyses can potentially provide information about how humans adapt to long-term, sustained climatic differences. Indeed, the negative relationship between geographical variation in temperature and suicide incidence hints at the presence of adaptation mechanisms to warmer temperatures that inhibit suicide risk in the long term. At the very least, this finding means that we should be cautious about assuming that the positive effect of irregular variation in temperature on suicide incidence implies that climate change will increase suicide risk. Until the reasons for the apparently conflicting effect of geographical variation in temperature can be identified, such an inference does not seem well justified.

Once again alarmist researchers doing an high wire act. Claims with virtually nothing to support them.
Footnote:
“Jumping the shark” is attempting to draw attention to or create publicity for something that is perceived as not warranting the attention, especially something that is believed to be past its peak in quality or relevance. The phrase originated with the TV series “Happy Days” when an episode had Fonzie doing a water ski jump over a shark. The stunt was intended to perk up the ratings, but it marked the show’s low point ahead of its demise.