Dr. Harvey Risch discusses how the Covid19 pandemic played out as a global disinformation campaign successfully inducing fear, uncertainty and doubt in the world’s populations. Thus authorities were able to exert unprecedented control over public behavior, with severe reductions of individual rights and freedoms.
Dr. Risch: Overall, I’d say that we’ve had a pandemic of fear, and the fear has affected almost everybody, whereas the infection has affected relatively few. It’s serious in some of those people, as we’ve seen. But by and large, it’s been a very selected pandemic, and predictable. We didn’t know at the beginning how predictable it was. At least we laypeople, so to speak, in the pandemic, didn’t know that.
I’m sure that the pharma companies and countries who had experienced it slightly before us had a better picture than we did, but it was very distinguished between young versus old, healthy versus chronic disease people. We quickly learned who was at risk for the pandemic and who wasn’t.
However, the fear was manufactured for everybody, and that’s what characterized the whole pandemic—is that degree of fear and people’s response to the fear.
I think that the people who were in the nominal positions of authority initially spread a much worse picture of the dire nature of this. That everybody was at risk, everybody could die, everybody needed to find protection. Everybody needed to stay in their homes and not go out, not socialize, and so on—to protect themselves [and] society.
People were quite afraid of that message as anybody would be, because one trusted in those times with the government, authorities, scientific people, medical people in authority, [and] the public health institutions all saying the same message starting in about February, March of last year.
So, we all kind of believed this, and therefore, all of our anxiety levels were raised, and we all made decisions to curtail, to various degrees, our exposures to other people—some more than others. But I think everybody had levels of anxiety that really affected how they carried out their life at that time.
Shock and Awe from China
Dr. Risch: We look at the videos that we got from Wuhan and the surrounding area in retrospect to see what was real about that, and what wasn’t. You have to recognize that almost every year there’s been an epidemic release from the live food markets in China, in various places. What was different about this one is that China has admitted to those right away and tried to fix them, whereas the present one, it did not do that.
It withheld information about it for two months, at least, and that withholding of information is a totally different behavior than how China has been in the past. That appears to be a very significant difference as to why it would do that. We know now that some of those videos were not truthful videos about that man falling over in the street and playing dead and things like that. We have reason to believe that those were artificial videos made to induce fear.
While the virus did get out in Wuhan and the lockdowns were there to suppress it, and they worked, in fact, when you suppress 100 percent of the population, you weld their doors shut and so on, you can do that. We’re not as draconian in the United States, at least haven’t been, and so it’s clear that the virus got out.
Whether there was an intention that it would be controllable on the local, but exportable to the rest of the world, is a risk-benefit equation that had to have been made in China at the time. In other words, China also faced the risk that this could get out and affect the whole country.
It did get to other places besides Wuhan, but I think they calculated that they would be able to control it better than we could. They also knew that chloroquine treated it because they had published on that five or more years in the past. We published on that too from NIAID at NIH, a paper on chloroquine and virus infections. I think it might’ve been SARS1 from 2005 that that was published, so we knew.
People knew. The scientific community knew that these viruses existed—that they were hazardous, they could be treated. But nobody knew exactly the extent, the ramifications of how well the treatment would work, whether that was enough by itself, what the hazards of using that drug were, what the long-term ramifications—all of that was still unknown territory.
War on Therapeutics
Dr. Risch: I started looking at the disparate information in medical and lay media about early treatment, and it just didn’t make sense that hydroxychloroquine was being badmouthed by the media when it was being studied in hospital patients, and saying that it didn’t work for outpatients when it hadn’t been studied in outpatients.
An outpatient disease is totally different from a hospital disease. It’s like night and day. Outpatient disease is like when you get the flu. You have fevers and chills and muscle aches, headache, sore throat, runny nose and cough. That’s a typical flu-like illness, outpatient.
Inpatient is a very severe pneumonia where the immune system debris fills up the lungs, and it’s a totally different disease. The virus is more or less long gone by that time, and it’s the immune system that’s overreacting to create that. So, it’s a different disease, requires different treatment, and yet, this was being pedaled as something that didn’t work in hospital disease, therefore it didn’t work in outpatient disease.
So, I wrote a paper looking at just hydroxychloroquine and remdesivir, which were the two agents that were being talked about in studies at the time in early-mid 2020, and I didn’t expect much to come out of that other than to say, “Look, here’s something that we could be using.”
I came into this. I wrote an op-ed for Newsweek saying, “Here it is. We should use it. There’s no cost, and even if it doesn’t work, it’s 100 percent safe because it’s been used in tens of billions of doses for 60 years in hundreds of millions of people. Even if it doesn’t work, it can’t do any harm.” Then I got pushback from my colleagues saying what do I know about infectious disease and epidemics and so on.
I’m a cancer epidemiologist, but they didn’t do their homework because after medical school I got a Ph.D. on mathematical modeling of infectious epidemics, and I published on that. I had a very clear idea of how epidemics come and go, and what herd immunity is, when it happens and how it happens, and all of that stuff.
The idea about using drugs to treat things is something that I do as just a regular part of my cancer epidemiology studies. So, this was not a great leap for me to be involved in these topics, and for them it was just smear. I didn’t respond to that, which is appropriate. They have their freedom of speech to say what they want to say. I have my freedom of speech to say what I want to say, and let the readers decide which seems the truest or the most accurate.
What Scientists Believe Vs. How Nature Behaves
Dr. Risch: I was thinking of cognitive dissonance. In other words, here I know it’s safe. At that time when I wrote the paper, there were five studies. Within another four or five months, there were 10 studies involving more than 40,000 patients who had been studied, including some national studies in Iran and Saudi Arabia—with tens of thousands of patients that provided very clear fivefold or better protection against mortality with this drug, and that’s not even using the recipe.
That’s just using hydroxychloroquine either by itself or with zinc, by and large, in these studies. It was very clear that the evidence was extremely strong, as strong of evidence as I’ve ever seen in anything in my career in epidemiology for an association, the magnitude of an association.
This is my bread and butter of the field that I understand and how it does these studies. What these studies were purporting to say was accurate, and a very strong signal. So I was nonplussed to find that people were saying, “These are anecdotal.” When Dr. Fauci would come in and say, “Oh, that evidence is anecdotal,” and I’m looking at 40,000 patients.
I’m looking at clinicians who’ve now treated more than 150,000 patients with fewer than two dozen deaths with hydroxychloroquine, and he’s saying it’s anecdotal, and I’m saying, “These 50 doctors all know that it’s not anecdotal. They’ve been using it in their practices for a year or a year-and-a-half.”
So, where is this disconnect? This disconnect has to be on purpose. It’s not an accident. It’s a smear campaign against the drug for a purpose.
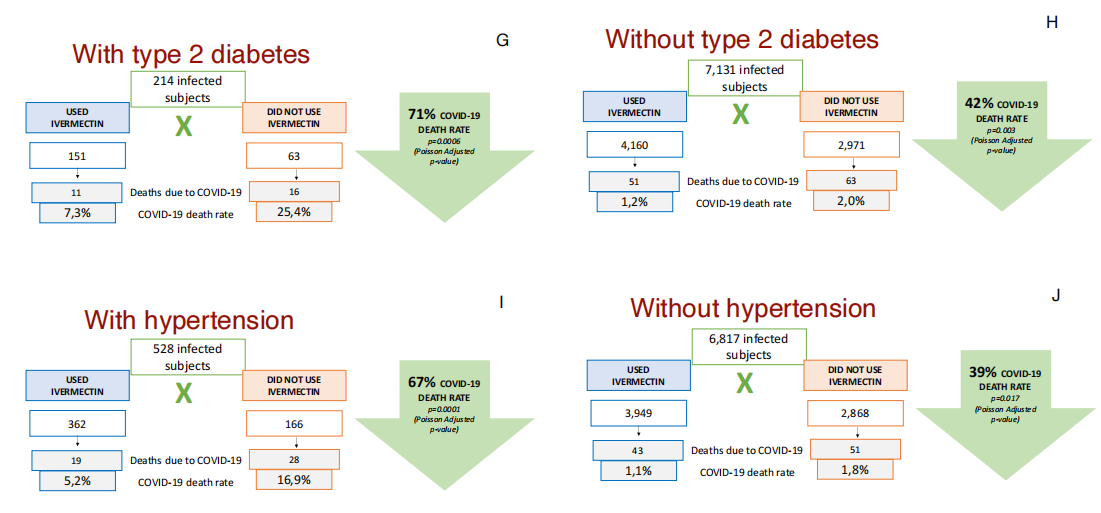
Where is the purpose coming from for why one would suppress something that costs 80 cents a day to treat? It’s even cheaper than ivermectin. Ivermectin is $10 a day or whatever it is. Hydroxychloroquine is a tenth of that.
You have to address what’s the economic playing field as to what is causing all of these events and all of these people to be making the arguments that they have, and in fact, without citing data? So, you find that people who disagree with me don’t provide counterevidence.
They say, “The FDA disagrees with you,” or, “The CDC disagrees with you,” or, “The WHO disagrees with you.” But is that evidence? Well, no, and in fact, Karl Popper, the philosopher of science in the 1950s, said studies of what scientists believe do not reflect on studies of how nature behaves.
Manipulation of Mortality
Dr. Risch: We believe that if the mortality numbers are accurate, and there are reasons not to believe that because as I said at the beginning, this has been an epidemic of fear, that agencies have magnified the fear component in order to control behavior.
People have conditions that aren’t really the cause of death that may or may not have been contributory, and this is a whole gray zone. COVID might’ve been the straw that broke the camel’s back, so to speak, or maybe it was just contributory.
We don’t really know the degree to which this was manipulated to make the numbers of deaths larger because of COVID than what really was some other rational way of calculating the numbers of deaths. It’s very hard to understand this. Even with the statistics that we have, it’s very hard to understand.
Dr. Risch: From October to October of 2020 to this year, I think there were 491 deaths in the five-to-11-year range with COVID. Now, that’s the problem. Kids in the hospital with some serious underlying condition that happened to be COVID-positive, that are asymptomatic and tested and found to be battling or infected with the virus, get called dying from COVID. But in fact, in the CDC’s own review slides, they say COVID-associated deaths.
Marty Makary at Johns Hopkins reported on the study from his institution of 48,000 children. He asserted that no healthy children in that study had died from COVID. So, that’s the real bottom line. Are we talking about zero or one or five across the country, or 10? We don’t really know exactly, but those numbers are smaller than the number of children who’ve died from influenza each year in past years when we’ve had flu epidemics, as we usually do, except for last year.
It’s a tenth of the number that die from traffic accidents. It’s lower than the number who get hit by lightning, and certainly lower than what flu does. So, why are we potentially forcing all children to get vaccinated to save approximately zero, since we know, we can tell who are the high-risk children? Why aren’t we vaccinating the high-risk children?
Disrupting the Process of Natural Immunity
People will argue every one of the things that I just said, but in fact, it’s very clear that children do perfectly well with this illness when they get it. Either they’re asymptomatic or they have a headache, they’re a little tired, they sleep a little long for a day or two, and that’s about it. That’s the extent of COVID in young children.
It’s not much different than a light flu or a cold in children, and that is probably how the illness is essentially meant to be manifested in a society where all children get it as little children, get through it without a big ruckus, and go on. Then everybody’s protected after that, and adults don’t have to worry about it because they all had it as children.
That’s most likely how this whole thing would work, but what happened now is we as immunologically naïve adults are exposed to this and react totally differently because we didn’t get it as children, and we don’t have that immunity. Well, some people do.
You have to explain why 75 percent, plus or minus, of people who’ve had COVID had it asymptomatically. That’s the adults who have had COVID. There’s a lot of immunity in the population because of all these people who’ve had it asymptomatically.
What that means is, when a state for example, reports that it’s had 200,000 cases per million, the people with COVID, that’s by testing. So, it’s either symptomatic or people who were screened and got tested. Two hundred thousand cases per million is 20 percent of the population has had COVID by testing or symptomatic. That means if you multiply that by five, essentially, everybody’s had COVID.
If that number is five, between three and seven, I’m just saying if it’s approximately five, then that’s the ballpark for estimating where the real immunity is, and that’s why you see states like North Dakota, South Dakota, other states that have minimal or no lockdowns, where everybody mixed, lots of people got COVID early.
People didn’t get very sick because they had relatively young, healthy populations that were doing most of the mixing, that they built up large amounts of population immunity, what we call herd immunity early on, and so they were largely done.
Now, Delta came. Some of the people, some of that natural immunity might have been not quite enough to deal with the Delta, so they’ve had a very small, low-level bump over the last few months that is probably going down also. But nothing like the states that locked down like Vermont and Hawaii and so on that spent all their time locked down, and with very severe curtailments of mixing.
And now are having these waves of pandemic that are bigger than what they first saw in early 2020 because it was misguided to try to suppress something that was going to be endemic no matter what anybody did.
The realization of when you take measures that just prolong the pandemic, it just gives it more time to build up, and you have more and more waves. If you let the pandemic go through the society in a controlled, safe way in the first waves, and you control how people respond to that infection in a way that minimizes their damage, their personal damage, you get through it, and that was the exact opposite.
That was what we were trying to say early on in April, May, June of 2020. You have to let this get through the population and develop natural immunity, and that is how we would solve it. That didn’t happen because of financial interests for selling products to deal with it instead of letting it happen on its own.
Front-line Doctors Discovered Viral Protection
Dr. Risch: Did people know how to deal with that? Yes and no. It wasn’t the right thing to do, but did they know what tools they might’ve had to set up shelters for infected elderly people instead of putting them back in nursing homes? I don’t know that people knew that was something they could do. They didn’t do that, but at the same time, we weren’t using the medications that could have been used that would’ve saved those people.
Elderly people have frail immune systems, and Dr. George Fareed in Southern California recognized early on that you can’t just give hydroxychloroquine and zinc and vitamin D and antibiotics day four or five, which works for middle-aged people perfectly well. Doesn’t work for frail elderly because the virus has had no immune system growing to try to suppress it because of their age and disabilities.
In them, you have to give it on day one. How do you give it on day one? It means you have to screen them daily. You screen them for a fever and pulse oximeters, the little toys that you buy at the Walgreens for $30, and you can test your blood oxygen levels, and doing that twice a day.
When those people, their oxygens were dropping but they weren’t otherwise symptomatic. Then you found that they already had a fever that you wouldn’t have recognized. You start treating them, and that’s what he did in nursing homes. He was very effective in saving the lives of people in nursing homes because he was getting to them on day one, and this kind of aggressive, safe method of treating people is what works and should’ve been done.
But it requires people who are willing to use what they know in classic medical practice, the way doctors were classically trained, which is each one is the Sherlock Holmes doctor of figuring out what you’re supposed to do and how it works and the best you can do, and treat the patients.
Not formulaic things that your hospital board or your medical practice board says, “These are the drugs you must use, and you can’t veer from this, and we’re telling you how to practice medicine.” Okay? That’s destroyed medicine.
There’s an academic disdain for local docs in general, that academics think that they are at the top of the medical/intellectual world because they’re doing their research, their clinical research. In some respects, it’s good, and for those areas that they actually study, that’s fine.
But for diseases on the front line, the doctors on the front line who are exploring, who are saying, “Well, this treatment works, but maybe I’ll try this in this patient, and that seemed to work a little better. Maybe I’ll try it in a few more patients,” and gradually accrete knowledge about how to treat things is the classical model for how diseases on the front line are managed.
That’s what worked for the doctors who are willing to do that in this pandemic, like all illnesses have dealt with in the past. That’s what brought the realm of knowledge to how we have treatment regimens.
Using a repurposed drug is perfectly reasonable if you believe, as a doctor based on the evidence, that you should use it, that you can try it, that you could help save someone’s life. I imagine that there was some kind of bigger influence or board or organization that would be setting such things. This has been my own learning process.
Medical Bureaucrats Failed in their Public Duty
Dr. Risch: I have to get in a comment about the FDA and its website. This is something that has made me the angriest over this last year-and-a-half. In July of 2020, the FDA mounted a website warning against hydroxychloroquine used for outpatients. The website’s still there.
It says, “Warning, hydroxychloroquine should not be used for outpatient treatments because of risk of cardiac adverse events,” and then in the small print, the fine print underneath that big, bold, black letter warning, it says, “We base this warning on adverse events that we have observed in hospital patients.” This is a fraud.
They used hospital disease, which all medical professionals recognize is a different disease, as I’ve said, than outpatient flu-like illness. That has stood up there. Everyone that says hydroxychloroquine can’t be used points to that website and says, “Here’s the reason why we can’t do it.” The states, the AMA, the pharmacy boards, they all point to that. Foreign countries, their governments all point to that, saying, “We can’t do it because the FDA says not to do it.”
I’ve railed against this in the media that we are a part of, and the way that the propaganda reacts to this is, “Ignore it. Ignore all of this.” I’m saying this now because the general public has to be the one that gets angry.
The general public should be furious at the way people have been treated in the country by suppression of these drugs, by that kind of website that suppresses the ability of doctors to practice medicine.
This is what should’ve been done, and why people should be angry. They should be angry at their government. They should be angry at President Trump for not leading the fight in this when he was in power. They should be angry at the government now for not leading the fight to make these drugs available. These drugs work, there’s no question, and they should’ve been out there, whether or not vaccines are used. There’s a role for vaccines, and I’m not saying that.
There’s no role for universal vaccination, but there is a role for targeted vaccination for people who have reasons to do the risk-benefit analysis and see it’s in their benefit. There’s a reason why those people will still get COVID, because the vaccines are not 100 percent effective.
They still need to have treatment, and these drugs are the treatments of choice. This has to be there, and people need to be angry about this to see why these drugs have been suppressed from them for reasons that have nothing to do with the science and the medicine.
HCQ or IVM protocols including nutritional supplements and antibiotics fill the need for early home treatment, whether people are vaccinated or not.








 Douglas W. Allen published a study
Douglas W. Allen published a study 





 Harvey Risch and Gerard Bradley write at Brownstone Institute
Harvey Risch and Gerard Bradley write at Brownstone Institute