Doctors of the World Unite Against Covid Tyranny

Doctors Uniting Around the World with Integrity and Right Action
More than 30,000 doctors and health care professionals have co-signed an Open letter published at the above website. Excerpts below in italics with my bolds. H/T Stephen Bird. World Doctors Alliance:
An independent non-profit alliance of doctors, nurses, healthcare professionals and staff around the world who have united in the wake of the Covid-19 response chapter to share experiences with a view to ending all lockdowns and related damaging measures and to re-establish universal health determinance of psychological and physical wellbeing for all humanity.
Open letter to the UK Government, Governments of the World and the Citizens of the World
We the undersigned call upon the UK government, governments of the World and the Citizens of the World, to stop all lockdown measures immediately.
Introduction
We were told initially that the premise for lockdown was to ‘flatten the curve’ and therefore protect the NHS from being overwhelmed.
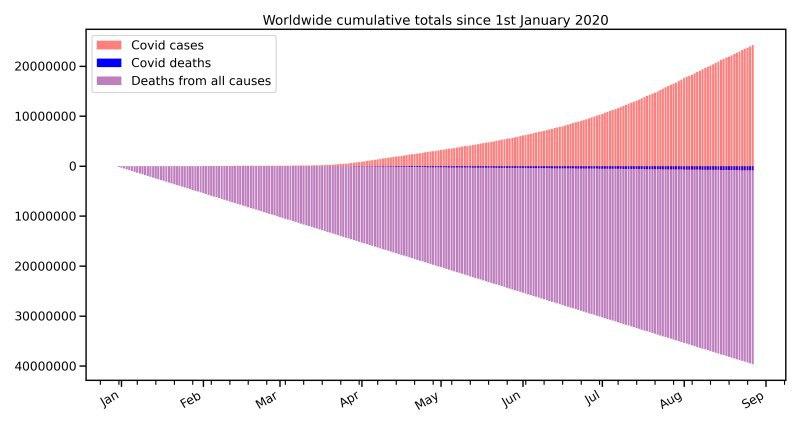
It is clear that at no point was the National Health Service (NHS) in any danger of being overwhelmed, and since May 2020 covid wards have been largely empty; and crucially the death toll from covid has remained extremely low.
We now have hundreds of thousands of so-called ‘cases’, ‘infections’ and ‘positive tests’ but hardly any sick people. Recall that four fifths (80%) of ‘infections’ are asymptomatic (1) Covid wards have been by and large empty throughout June, July, August and September 2020. Most importantly covid deaths are at an all-time low. It is clear that these ‘cases’ are in fact not ‘cases’ but rather they are normal healthy people.
So-called asymptomatic cases have never in the history of respiratory disease been the driver for spread of infection. Rather it is symptomatic people who spread respiratory infections – not asymptomatic people.(2)
It is also abundantly clear that the ‘pandemic’ is basically over and has been since June 2020. (3)
We have very highly likely reached herd immunity and therefore have no need for a vaccine.
We have safe and very effective treatments and preventative treatments for covid, we therefore call for an immediate end to all lockdown measures, social distancing, mask wearing, testing of healthy individuals, track and trace, immunity passports, the vaccination program and so on.
There has been a catalogue of unscientific, non-sensical policies enacted which infringe our inalienable rights, such as – freedom of movement, freedom of speech and freedom of assembly. These draconian totalitarian measures must never be repeated.
Lockdown
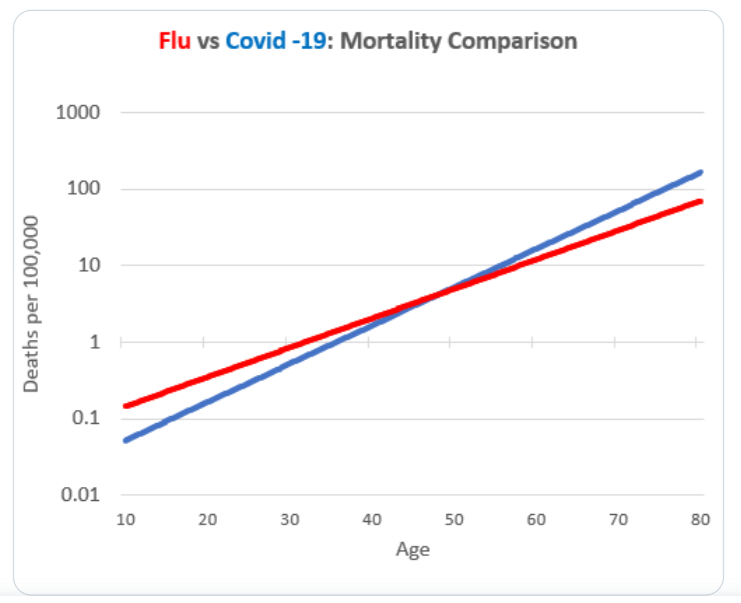
Covid has proved less deadly than previous influenza seasons – There were 50,100 flu deaths from December 2017 to March 2018 in England and Wales. There were 80,000 flu deaths in 1969. To date we have circa 42,000 covid related deaths in the UK.
We have never locked down society for a respiratory virus before.
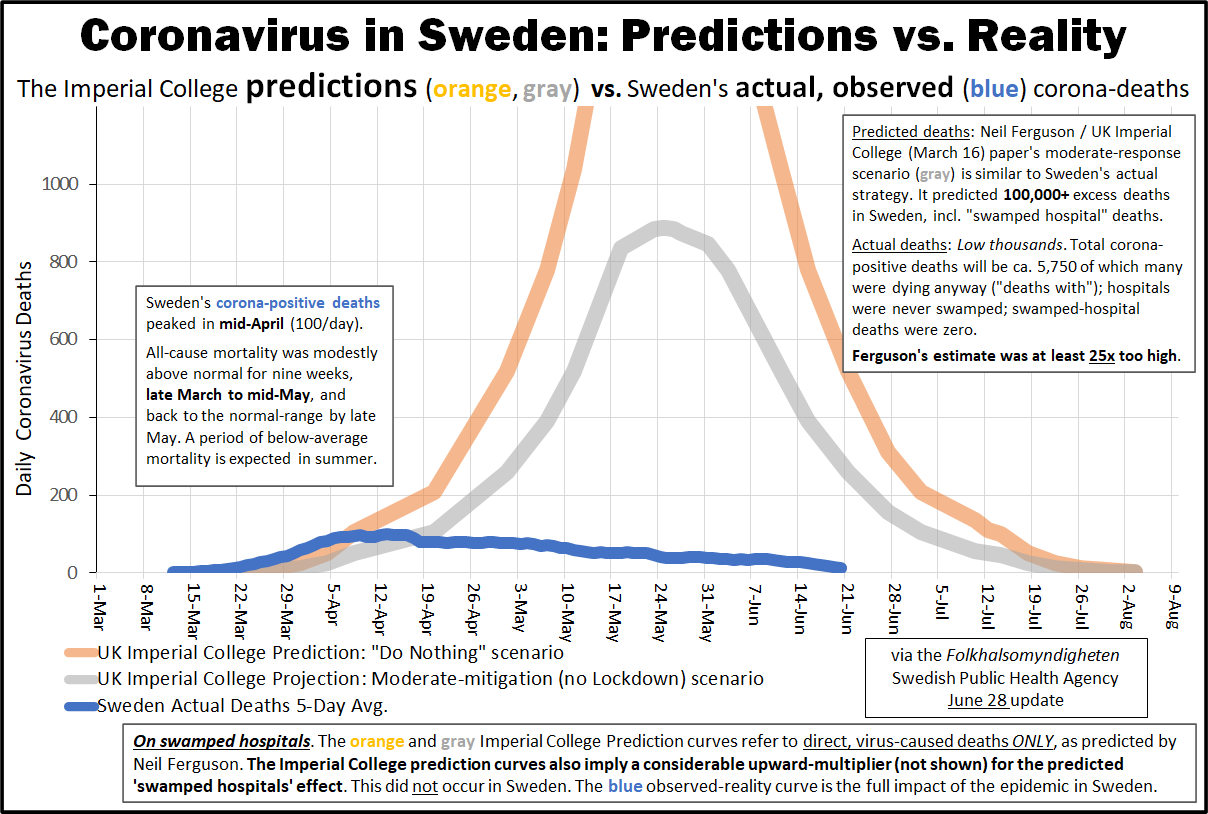
The basis for lockdown was a mathematical model by Professor Neil Ferguson. His modelling which predicted half a million deaths in the UK has been roundly condemned as being not fit for purpose. His estimated death figures were clearly wrong by a factor of 10 or 12 times. (1)
Professor Ferguson’s modelling was not even peer reviewed before being acted upon by several nations. Eminent epidemiologists such as Professor Gupta from Oxford University were ignored, they estimated the death count would be far lower in the UK.
Professor Ferguson has a long track record of woeful modelling he was entirely wrong about sars, mers, mad cow’s disease (CJD), and swine flu. Why did the world listen to him again? (2)
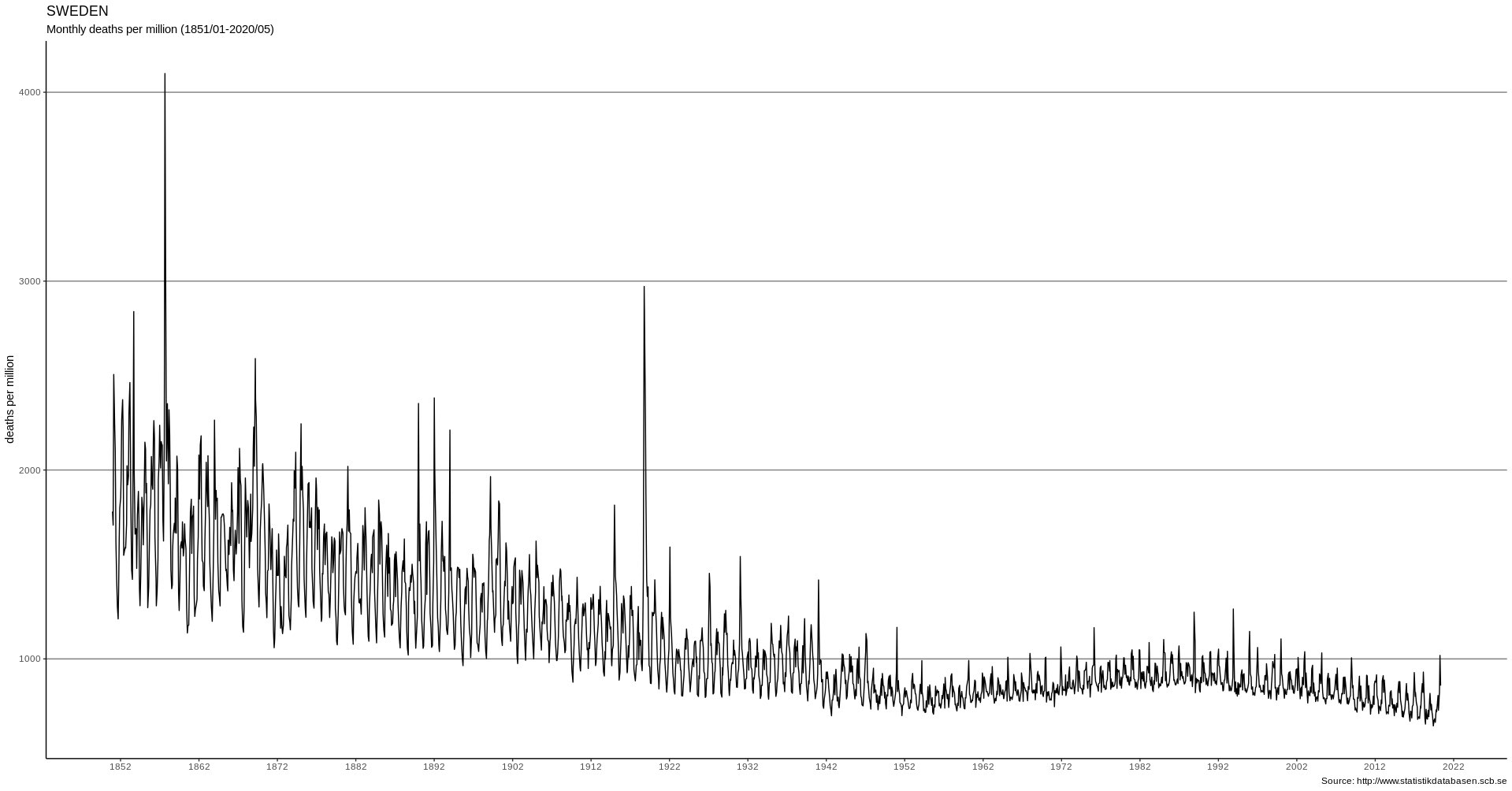
Countries which did not lock down Sweden, Japan, Taiwan, South Korea and Belarus have all done significantly better than us in terms of percentage of population deaths. They also have herd immunity and intact economies.
Lockdown did not save lives, and this has been published in the Lancet ‘….in our analysis, full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.’ (3)
The vast majority of deaths occurred in elderly and very elderly people
The vast majority of deaths occurred in people with pre-existing serious health issues such as cancer, cardiovascular disease, Alzheimer’s, diabetes etc
Covid poses virtually zero risk to the under 45’s who have more chance of being struck by lightning than dying from covid.
Covid poses a very small risk for healthy under 60 year olds who have a greater chance of accidental drowning than dying from covid.
The entire nation was essentially placed under house arrest. We have never isolated the healthy before.
Isolating the sick and those who are immunocompromised makes sense. Isolating the healthy has hampered the establishment of herd immunity and makes no sense.
To put it into perspective we had 115,000 smoking related deaths in the UK in 2015 compared to the 42,000 deaths from covid.
We usually have around 600,000 deaths every year in the UK, roughly 1600 deaths per day.
Collateral Damage: The Cure is Worse than the Virus
Placing the public under virtual house arrest has caused untold damage to both physical and mental health.(1)
Ventilating patients instead of oxygenating patients proved to be a deadly policy and an unwarranted failure. Ventilation resulted in many unnecessary deaths. (2)
Sending infected people from hospitals to care homes placed the elderly and frail under unnecessary risk and resulted in many unnecessary deaths. (3)
Blanket Do Not Resuscitate (DNR) orders were imposed on thousands of people without their consent nor the consent of their families – this is both unlawful and immoral and lead to unnecessary deaths in care homes. (4)
Hospitals became essentially ‘covid only’ centres vast numbers of patients were wilfully neglected, resulting in many thousands of unnecessary deaths. (5)
The government’s own report estimates that some two hundred thousand (200,000) people will die as a direct result of lockdown – not the virus. Hospitals being closed, suicide and poverty will result in more deaths than the virus. (6)
The cure is worse than the disease!
[Other Topics covered in the declaration include:
- Death Certificates
- Economic Ruin
- Censorship
- Testing–False Positives
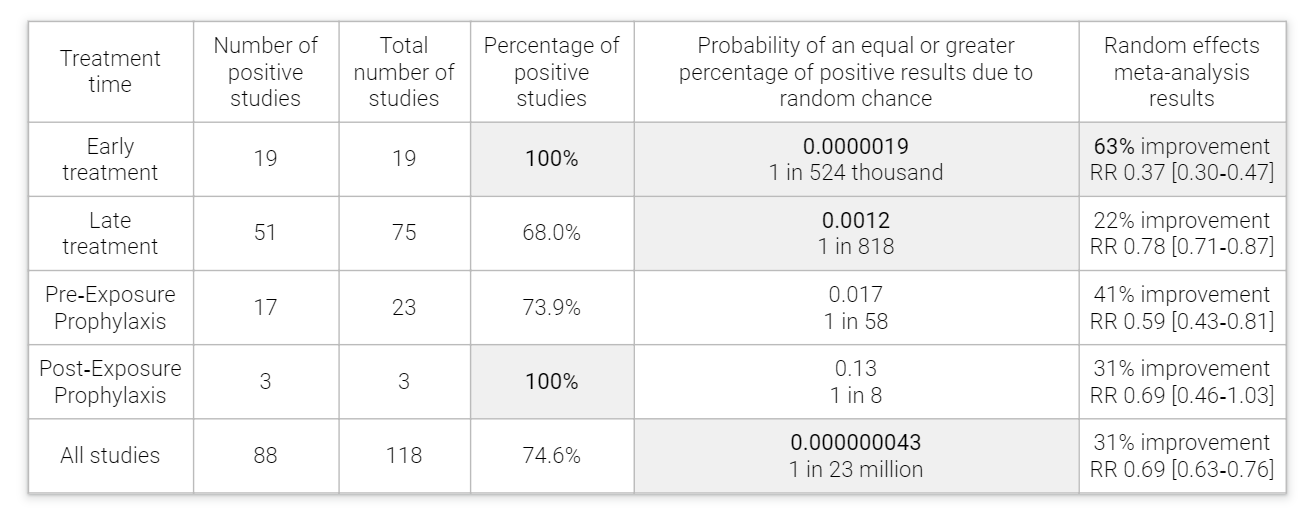
- Hydroxychloroquine
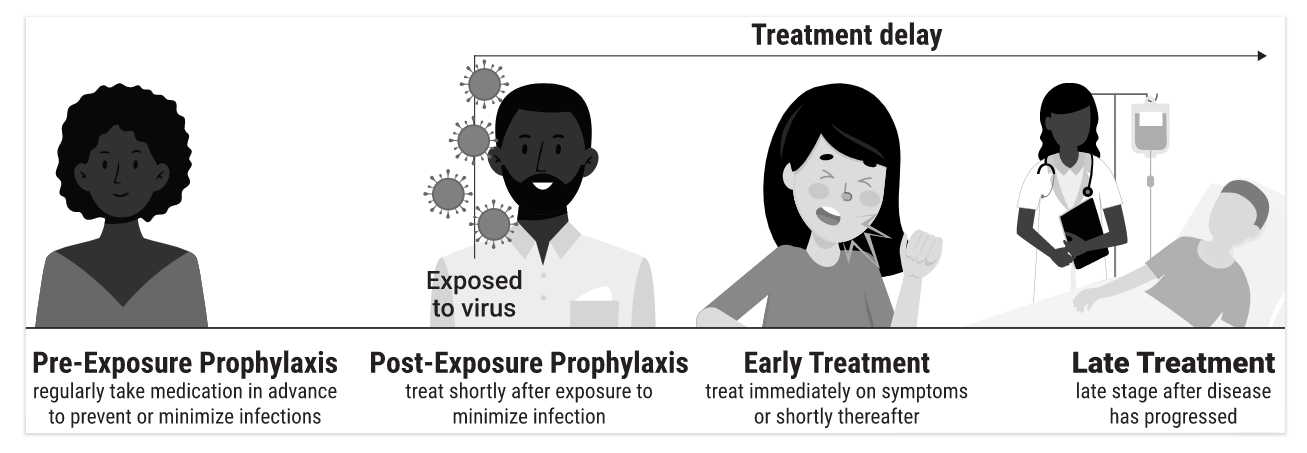
- Prevention
- Vaccine
- Conflicts of Interest
- Cui Bono? Who Benefits?
Conclusion
We have effective and safe treatments and preventative medications for covid, therefore there is no need for any lockdown restrictions and associated measures. The pandemic is essentially over as can be seen by the consistent low death rate and hospital admissions over the past four months.
We demand the immediate and permanent ceasing of all lockdown measures.
Lockdowns do not save lives, that is why they have never been used before. Civil liberties and fundamental freedoms have been unnecessarily removed from the public and this must never happen again.
Preventative measures such as Hydroxychloroquine, vitamin C, Vitamin D and zinc must be made readily available to the public.
Isolation must be voluntary. People are perfectly capable of making their own assessment of the risks and must be free to go about their lives as they so choose. People must have the right to choose whether to isolate or not.
Likewise, businesses must have the right to remain open if they so choose.
We demand that doctors, nurses, scientists and healthcare professionals must be permitted free speech and never be censored again.
Professor Mark Woolhouse epidemiologist and specialist in infectious diseases, Edinburgh University Member of the Scientific Pandemic Influenza Group on Behaviours, that advises the Government stated that –
‘…Lockdown was a monumental disaster on a global scale. The cure was worse than the disease.’
‘I never want to see national lockdown again. It was always a temporary measure that simply delayed the stage of the epidemic we see now. It was never going to change anything fundamentally, however low we drove down the number of cases,’
‘We absolutely should never return to a position where children cannot play or go to school.’
I believe the harm lockdown is doing to our education, health care access, and broader aspects of our economy and society will turn out to be at least as great as the harm done by Covid-19.’(1)
The World Doctors Alliance agree fully with Prof Woolhouse’s assertions, he is right! We must never lockdown again!





 Jeffrey A. Tucker writes at AIER American Institute for Economic Research
Jeffrey A. Tucker writes at AIER American Institute for Economic Research