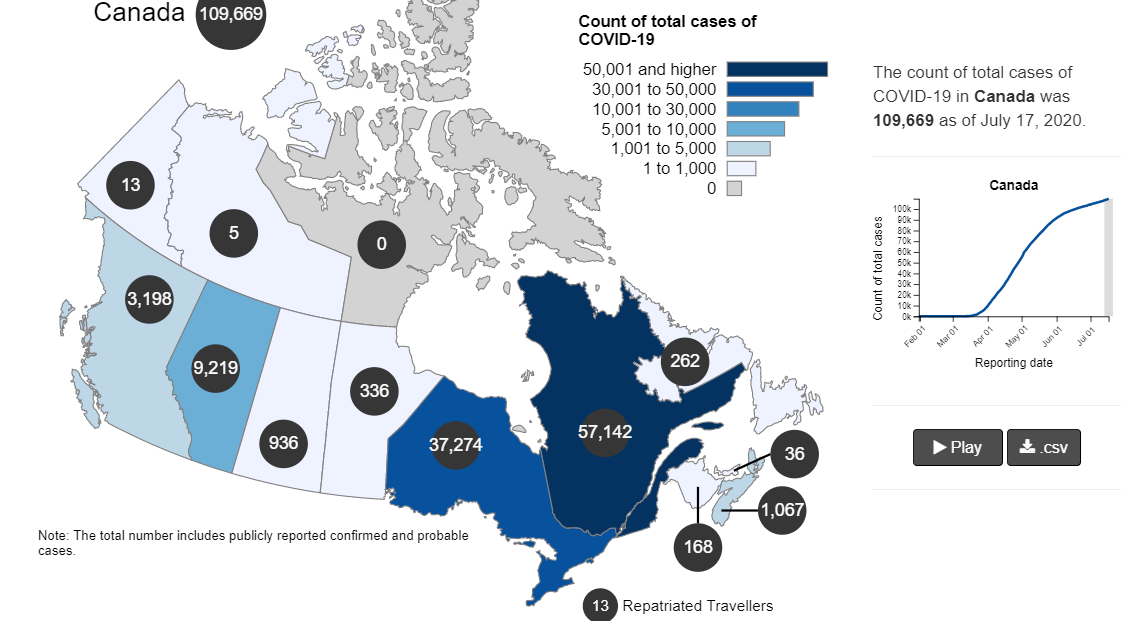
The map shows that in Canada 8929 deaths have been attributed to Covid19, meaning people who died having tested positive for SARS CV2 virus. This number accumulated over a period of 182 days starting January 31. The daily death rate reached a peak of 177 on May 6, 2020, and is down to 7 as of yesterday. More details on this below, but first the summary picture. (Note: 2019 is the latest demographic report)
Canada Pop
Ann Deaths
Daily Deaths
Risk per Person
2019
37589262
330786
906
0.8800%
Covid 2020
37589262
8929
49
0.0238%
Over the epidemic months, the average Covid daily death rate amounted to 5% of the All Causes death rate. During this time a Canadian had an average risk of 1 in 5000 of dying with SARS CV2 versus a 1 in 114 chance of dying regardless of that infection. As shown in a previous post, the risk varied greatly with age, much lower for younger, healthier people.
The Key Covid Metric
With easing of lockdowns and increased testing in many places, epidemiologists are focusing on a key metric to inform public policies: Positivity. The positivity metric is the rate (%) of people who test positive out all people sampled. The significance is that (by definition) a presumed case is a person who tests positive once. If a second test comes back positive it is a confirmed case. The metric is not perfect for two reasons.
The first problem is false positives from the testing procedure itself or from errors in the data processing and reporting. For this we have to hope that quality assurance protocols are being followed and mistakes corrected along the way.
The larger issue appeared in Florida recently when officials discovered that numerous batches of samples were reported 100% positive and other batches 100% negative. While the latter result is expected sometimes, all people testing positive seems unlikely. Behind this is the reality that in many situations (eg hospital ICU) a single patient will be tested many times with many positive results in the course of monitoring that individual’s clearing of the virus. Obviously a batch of samples from that ICU might legitimately be 100% positive.
But it is also true that 10 or 20 positive tests from one patient should not be reported as 10 or 20 new cases. In some jurisdictions, officials say they go to the effort to link test results to the individuals tested, and can distinguish between number of cases and number of positives. In other places, cases and positives may be the same number. Thus confirmed cases could be only 1/2 of the total positives, or less.
How is Canada Doing?
Because of some irregularities in national data reporting, this update is based on Ontario and Quebec statistics combined. Together the two provinces account for 72% of national testing, 85% of cases and 95% of deaths after testing positive for Covid19. Like many places, the Canadian contagion is not a pandemic, but rather a few hot spots within a largely untouched geography, This post is reporting the two central provinces as representing the Canadian epidemic. Quebec data is here: https://www.inspq.qc.ca/covid-19/donnees. Ontario data is here: https://covid-19.ontario.ca/data.
The line shows the Positivity metric for Canada starting at nearly 10% for new cases April 22, 2020. That is, for the 7 day period ending April 22, there were a daily average of 13225 tests and 1283 new cases reported. Since then the rate of new cases has dropped down, now holding steady at ~1% for the last month. Yesterday, the daily average number of tests was 35,747 with 274 new cases. So despite 2.7 times the testing, the positivity rate is not climbing.
Another view of the data (all Canadian provinces) is shown below.
Note that increased testing has led to a slight bump in new cases, but the positivity rate is little changed. Meanwhile, the death rate has continued to decline from a high of 177 on May 6 down to 7 deaths presently.
Meanwhile the national messaging focuses on rising cumulative case totals, ignoring evidence the contagion is winding down.
My bad. That is the Health Minister of PEI solemnly announcing in July their first Covid case in two months.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused the rapidly unfolding coronavirus disease 2019 (COVID-19) pandemic1,2 . Clinical manifestations of COVID-19 vary, ranging from asymptomatic infection to respiratory failure. The mechanisms determining such variable outcomes remain unresolved. Here, we investigated SARS-CoV-2 spike glycoprotein (S)-reactive CD4+ T cells in peripheral blood of patients with COVID-19 and SARS-CoV-2-unexposed healthy donors (HD). We detected SARS-CoV-2 S-reactive CD4+ T cells in 83% of patients with COVID-19 but also in 35% of HD. S-reactive CD4+ T cells in HD reacted primarily to C-terminal S epitopes, which show a higher homology to spike glycoproteins of human endemic coronaviruses, compared to N-terminal epitopes. S-reactive T cell lines generated from SARS-CoV-2-naive HD responded similarly to C-terminal S of human endemic coronaviruses 229E and OC43 and SARS-CoV-2, demonstrating the presence of S-cross-reactive T cells, probably generated during past encounters with endemic coronaviruses. The role of pre-existing SARS-CoV-2 cross-reactive T cells for clinical outcomes remains to be determined in larger cohorts. However, the presence of S-cross-reactive T cells in a sizable fraction of the general population may affect the dynamics of the current pandemic, and has important implications for the design and analysis of upcoming COVID-19 vaccine trials.
Discussion
Our study demonstrates the presence of S-reactive CD4+ T cells in COVID-19 patients, and in a considerable proportion of SARS-CoV-2 unexposed HD. In light of the recent emergence of SARS-CoV-2, our data raise the intriguing possibility that such pre-existing S-reactive T cells represent cross-reactive clones, probably acquired in previous infections with endemic HCoVs. HCoVs account for approximately 20% of “common cold” upper respiratory tract infections, are ubiquitous, but display a winter seasonality30–32. Based on epidemiological data, it may be extrapolated that adults contract an HCoV infection on average every two to three years. Protective antibodies may wane mid-term but cellular immunity could remain13,33. Although the overall amino acid sequence homology of S is relatively low compared to spike glycoproteins of HCoVs, there is an overlap of MHC-II epitopes especially in the C-terminal domain of the here used peptide pools (Fig. 1a, Extended Data Fig. 1). This may explain the preferential reactivity of CD4+ T cells to the C-terminal domain in one third of HD.
The biological role of pre-existing S-cross-reactive CD4+ T cells in 35% of HD remains unclear for now. However, assuming that these cells have a protective role in SARS-CoV-2 infection, they may contribute to understanding the divergent manifestations of COVID-19, and the striking resilience of children and young adults to symptomatic SARS-CoV-2 infection. Especially children in day care centers but also young adults have more frequent social contacts than elderly, and thus may have a higher HCoV prevalence. This hypothesis requires further investigation in future longitudinal studies assessing the presence of pre-existing SARS-CoV-2-cross-reactive CD4+ T cells and their impact on the susceptibility to SARS-CoV-2 infection and age-related clinical outcomes of COVID-19.
SARS-CoV neutralizing antibodies are associated with convalescence, and they have been detected 12 months after disease9 . However, the durability of neutralizing antibody responses against SARS-CoV-2 remains unknown. Although antibodies against HCoV can wane within months after infection, HCoV re-infection is accompanied by low-level and short-lived virus shedding with only mild symptoms of short duration pointing towards humoral-independent residual immunity10. Cellular immunity has not yet been studied in this context. In mouse models, however, CD4+ as well as CD8+ T cell responses directed against structural proteins such as spike or nucleocapsid protein of SARS-CoV critically contributed to viral clearance15,34,35. Understanding the extent to which and how SARS-CoV-2-specific humoral or cellular immunity mediates durable protection against reinfection is of critical importance in the coming months.
Our study reveals pre-existing cellular SARS-CoV-2-cross-reactivity in a substantial proportion of SARS-CoV-2 seronegative HD. This finding might have significant epidemiological implications regarding herd immunity thresholds and projections for the COVID-19 pandemic. Our results provide a decisive rationale to initiate worldwide prospective studies to assess the contribution of pre-existing, potentially region-dependent SARS-CoV-2-cross-reactive immunity to the diverse clinical outcomes of SARS-CoV-2 infections. Together with currently introduced novel serological tests, the data generated by such studies may critically inform evidence-based risk evaluation, patient monitoring, adaptation of containment methods, and last but not least, vaccine development.
Don’t Fence Me In!
Implications of This Research are explained in a previous post Herd Immunity Already?
Professor Sunetra Gupta provides a wise, wholistic perspective on the pandemic in her interview published at Reason We may already have herd immunity. Excerpts in italics with my bolds. H/T Paul Yowell.
I particularly appreciate her sense of the complexity of multiple factors and values, and humility in the challenge of getting the balance right. This contrasts with so many narrow and overly confident technical pronouncements we read and hear in the media.
Are we already immune to coronavirus? Professor Sunetra Gupta, a theoretical epidemiologist at Oxford University, discusses her recent study on the herd immunity threshold, as well as her views on the social costs of lockdown, the inaccuracy of epidemiological models, and the curtailment of academic debate.
A study produced by a team at Oxford University indicated that some parts of the United Kingdom may already have reached herd immunity from coronavirus. A significant fraction of the population, according to the study published last week, may have “innate resistance or cross-protection from exposure to seasonal coronaviruses”, making the proportion vulnerable to coronavirus infection much smaller than previously thought.
The Oxford team is led by Sunetra Gupta, a professor of theoretical epidemiology. In recent months, she has argued that the cost of lockdown will be too high for the poorest in society and questioned the language and quality of debate on the pandemic’s impact.
Reaction interviewed Professor Gupta about these matters and more, with questions from Maggie Pagano, Alastair Benn and Mutaz Ahmed.
Cross-immunity Matters
Yes, exactly. The principle of protection from exposure to related viruses, and indeed any kind of pathogen, is one that we’ve known for a very long time. The very first vaccine we had, which is smallpox, was based on the idea that cowpox protects against smallpox. This idea was already there well in advance of us knowing that smallpox was a virus – and indeed in advance of germ theory having been properly established. So we knew about this cross protection even before we knew that diseases were caused by germs. It’s a very old idea.
In my own studies, beginning with malaria and then later thinking about flu, the role of cross-immunity in protecting against disease seemed to be something that very much needed to be factored into our thinking. Most of the people who die from malaria are children, and they die upon their first exposure, because they have no immunity at that stage. That was one of the first things that struck me when I was working on malaria.
And then later when I was working on flu, it seemed to me a very good way of explaining why the 1918 flu had killed so many people, but why that didn’t seem to be repeating itself, was that it was likely that people hadn’t been exposed to flu. Many people would have not had the flu at all. So then that built up this population of naive immunity in people under the age of thirty who were very badly affected when the pandemic came through.
Having those ideas in mind, when the Covid-19 virus started to spread, I was pretty certain it wouldn’t have a huge, devastating impact in terms of mortality, because we had all these other coronaviruses circulating.
What I didn’t anticipate was that some of our responses to previous exposure to seasonal coronaviruses might actually protect us from infection. It’s one thing to get infected and not ill, but what the new studies are showing is that people are actually fighting off infection. So at an even more basic level, the pre-existing antibodies or T-cell responses against coronaviruses seem to protect against infection, not just the outcome of infection.
Low Seroprevalence May be a Good Thing
What we know is that the seropositivity rates in many parts of the world are much lower than we’d expect them to be if we assume that the epidemic has passed through and that people are resistant. If you take a very simple scenario where everyone is susceptible, you’d expect 60-70% of them to have some marker of exposure. And that is not what’s been observed.
One of the things that’s been done in reporting the seroprevalence, which is not correct, is that they’ve been homogenised. When people say only 5-6% of the UK population has been exposed, that’s not correct. I think very few people would agree that exposure rates in London are less than 20%.
The picture that we’re getting is heterogeneous. But even in hotspots, apart from a few reports, they’re still quite low. So why is that?
One reason might be that lockdown stopped the spread of infection, so it was halted at a stage when, say, 20% of people were immune and the rest of the people were still susceptible to infection. Well, under those circumstances, the easing of lockdown should result in fairly rapid growth of cases. And that’s not something we’re seeing.
So we’ve got those two bits of information. The third bit, the missing piece of the puzzle, is this idea that some people are fully resistant to infection, because they just have really good defences. That could just be part of our innate immunological makeup. It’s also becoming clear that some of the people that have beaten it off have had responses to other coronaviruses which could have played a role.
The other bit of the puzzle is that some people do get infected and they make antibody responses, but those responses die very quickly. So if you’re trying to measure exposure, you won’t get the full picture. Some of the measures of seroprevalence might be underestimates.
We’ve got four pieces of the puzzle, then. If we put them all together, which is what the paper that we published on Friday does, it gives you a theoretical framework that you can use to look at how these bits connect up together.
You can see two things. You can see why the seroprevalence level might be low, and you can also infer that the level of herd immunity needed to stop the thing from exploding again is actually much lower than the figures that are currently being thrown around quite incautiously might suggest.
The fifth piece of this jigsaw could be that there is some seasonality. I suspect that in the winter it will probably come back, but hopefully only to the regions where it was kept from going by lockdown, and where the seroprevalence levels are genuinely extremely low.
We can be cautiously hopeful that in areas where the seroprevalence levels have achieved a certain value that’s compatible with there being a proportion who are resistant, that it might not come back with such vehemence.
Quality of Life Matters
What’s disappointed me about the way this has been approached is it has been approached along a single axis, which, if you like, is a scientific one. Even within that context, you could argue that it’s too one-dimensional, so we’re not thinking about what’s happening with other infectious diseases or how many people are going to die of cancer.
That’s the axis of disease, but then there’s the socioeconomic axis, which has been ignored. But there’s a third, aesthetic access, which is about how we want to live our lives. We are closing ourselves off not just to the disease, but to other aspects of being human.
I think the trade-off is very extreme. Obviously the most extreme manifestation of that trade-off is the 23 million people who will be pushed below the poverty line as a result of this sledgehammer approach. The costs to the arts is I think also incredibly profound – the theatres and all other forms of performing art. But also the inherent art of living, which I think is being compromised.
Acts of kindness are being eschewed. Someone was telling me yesterday that their mother said to them “please don’t come home, you’re going to kill us”.
Carrying On with Living is Social Responsibility
Because actually, the only way we can reduce the risk to the vulnerable people in the population is, for those of us who are able to acquire herd immunity, to do that.
Even if there is a little bit of a risk. I’m 55 years old, there’s some slight risk out there. But I would be willing to take that, just as I do with the flu. There’s a risk I might die of flu, but I’m willing to take that risk, because I know that if I don’t then flu will appear as it did before, it will enter the population of immunologically naive individuals, and then there will be a high risk of infection which will have a disproportionate effect on the vulnerable sector of the population.
Maybe the way to counter it now is to say, actually, not only is it a good thing for young people to go out there and become immune, but that is almost their duty. It’s a way of living with this virus. It’s how we live with other viruses. Flu is clearly a very dangerous virus, but the reason we don’t see more deaths from flu every year is because, through herd immunity, the levels of infection are kept to as low a level as we can get.
The truth is that herd immunity is a way of preventing vulnerable people from dying. It is achieved at the expense of some people dying, and we can stop that by preventing the vulnerable class in the process. In an ideal situation, you would protect the vulnerable as best you can, let people go about their business, allow herd immunity to build up, make sure the economy doesn’t crash, make sure the arts are preserved, and make sure qualities of kindness and tolerance remain in place.
We live, it seems, in this state of terror. Yes, international travel facilitates the entrance of contagion, but what it also does is it brings immunity.
Good Thing It’s Not Our First Coronavirus
If coronavirus had arrived in a setting where we had no coronavirus exposure before, we might be much worse off. It also seems that in addition to protection against severe disease as a result of exposure to related coronaviruses, some fraction of us seem to be resistant to infection.
That’s just fantastic news, actually. Hopefully that will be consolidated at a scientific, laboratory level. We ourselves are looking at how antibodies to seasonal coronaviruses can impact on protection against infection and disease.
Maybe we will be able to build up a picture that will reassure the public that actually we are much better off having been exposed to related coronaviruses. We are in a better place to fight off this infection than we actually thought.
Abstract It is widely believed that the herd immunity threshold (HIT) required to prevent a resurgence of SARS-CoV-2 is in excess of 50% for any epidemiological setting. Here, we demonstrate that HIT may be greatly reduced if a fraction of the population is unable to transmit the virus due to innate resistance or cross-protection from exposure to seasonal coronaviruses. The drop in HIT is proportional to the fraction of the population resistant only when that fraction is effectively segregated from the general population; however, when mixing is random, the drop in HIT is more precipitous. Significant reductions in expected mortality can also be observed in settings where a fraction of the population is resistant to infection. These results help to explain the large degree of regional variation observed in seroprevalence and cumulative deaths and suggest that sufficient herd-immunity may already be in place to substantially mitigate a potential second wave.
H/T Palmer Foundation (here) for transcript synopsis, printed in italics with my bolds.
A Nigerian-born and trained physician, Dr Stella Immanuel, is trending on social media after delivering an impassioned COVID-19 speech in the U.S.
That was until U.S. President Trump retweeted it. Now the video is being removed from all over the internet. Facebook has gone so far as to completely remove her account.
Speaking at a news conference in Washington, Immanuel claimed that antimalarial drug, hydroxychloroquine, zinc, and antibacterial drug, Zithromax, were effective cures for the virus.
She said she had successfully treated no fewer than 350 patients with hydroxychloroquine, zinc, and Zithromax.
The following are excerpts of Immanuel’s speech:
“Hello, I’m Dr Stella Emmanuel. I’m a primary care physician in Houston, Texas.
“I went to medical school in West Africa, Nigeria, where I took care of malaria patients, treated them with hydroxychloroquine and stuff like that.
“So I’m used to these medications. I’m here because I have personally treated over 350 patients with COVID-19. Patients that have diabetes, patients that have high blood pressure, patients that have asthma, old people … I think my oldest patients are 92 … 87-year-olds.
“And the result has been the same. I put them on hydroxychloroquine, I put them on zinc, I put them on Zithromax, and they’re all well. For the past few months, after taking care of over 350 patients, we’ve not lost one. Not a diabetic, not a somebody with high blood pressure, not somebody who asthma, not an old person.
“We’ve not lost one patient. And on top of that, I’ve put myself, my staff, and many doctors that I know on hydroxychloroquine for prevention because by the very mechanism of action, it works early and as a prophylaxis.
“The study that made me start using hydroxychloroquine was a study that they did under the NIH in 2005 that says it works.
“I know you’re going to tell me that you treated 20 people, 40 people, and it didn’t work. I’m a true testimony. So I came here to Washington DC to tell America nobody needs to get sick.
“This virus has a cure. It is called hydroxychloroquine, zinc, and Zithromax. I know you people want to talk about a mask. Hello? You don’t need a mask. There is a cure.
“I tell all of you doctors that are sitting down and watching Americans die. You’re like the good Nazi … the good one, the good Germans that watched Jews get killed and you did not speak up.
“If they come after me, they threaten me. They’ve threatened to … I mean, I’ve gotten all kinds of threats. Or they’re going to report me to the bots.
“I say, you know what? I don’t care. I’m not going to let Americans die. And if this is the hill where I get nailed on, I will get nailed on it. I don’t care.
“And today I’m here to say it, that America, there is a cure for COVID-19. All this foolishness does not need to happen. There is a cure for COVID-19.
My Comment:
Dr. Immanuel is not alone, and was speaking along with a group of frontline doctors who have had similar experience as Covid caregivers. There are those already dismissive of HCQ treatments, unless and until there is incontrovertible double blind large scale trials. In fact the bad press exaggerating HCQ risk factors makes recruiting trial volunteers nearly impossible, and maybe that was the intention. Of course also being an evangelical preacher is an easy target for cancellation, despite her being an outspoken black woman.
Abuja, July 28, 2020 The Guild of Medical Directors (GMD) has reacted to video claims by Dr Stella Immanuel, a General Practitioner (GP) in the U.S. that she has treated over 350 patients of COVID-19 with combination of Hydrochloroquine (HCQ), Zinc and Zithromax, saying it is her own personal, unsubstantiated claim.
In a statement seen by Naija247news from the President of GMD, Prof. Olufemi Babalola in Abuja on Tuesday, the doctors said “there is no scientific evidence to prove the claim.”
The guild president noted that while some studies suggested that it was effective, others felt otherwise.
He added that “it is true that Senegal, where HCQ is routinely used, has one of the lowest COVID-19 case fatality rates in the world at 0.64 per cent compared to 3.4 per cent in the U.S.
“As we speak, a study is underway at Lagos University Teaching Hospital (LUTH) on its efficacy and safety. Subsequently, a meta-analysis of all these studies should be undertaken to pool all the results and come up with analysis which will guide clinicians.
“So, until then, all anecdotal claims such as the one from Dr Stella Immanuel must be taken with a pinch of salt.”
The observation about Senegal also shows why the HCQ treatment is worth pursuing.
Consider this chart produced in early June.
Now that is only suggestive, not proven association because inter-country comparisons have many complicating factors, and case fatalities change over time and with greater data collected. Still, it indicated that places that use HCQ routinely appeared to have lower lethality compared, for example, to Europe which mostly followed WHO’s position discouraging HCQ. Other national experiences are compelling:
Algeria – Started using Chloroquine in late March. Results came very soon
According to one infectious disease specialist, “near-total effectiveness.”
Morocco – Also started treating in late March
Again, almost immediate results
Fun fact: more people have died of COVID in the Moroccan diaspora than in Morocco! Think about that for a second…
Conclusion:
Yes, they will go after Dr. Immanuel and cancel her if possible. But this is much bigger than her.
“Florida Sets Yet Another Coronavirus Record: 173 Deaths In A Day.”
“A record 173 Floridians died from the virus Thursday, an average of more than one every eight minutes.”
“The 134 new confirmed deaths is the second-largest increase on record, coming five days after the largest one-day jump of 156 last week.”
“COVID-19 has ravaged Florida, with more than 237,000 people testing positive and 2,013 dying from the virus in July alone.”
So what characteristic do all of the reports share? They are all false.
It is not true that 173 people died from COVID-19 “in a day” in Florida. Nor did 134, or 156 on previous days.
It is also untrue than 2,013 had died in July when that story was published.
All of these scary headlines are based on the number of deaths reported by the state on any given day. This is not the same as the number of deaths that occurred on those days.
The difference might seem trivial. But it’s crucial because the press is using the timing of Florida’s death reports to whip up a frenzy about COVID-19 running riot in the state.
Take a look at the chart below. The blue bars are the number of deaths reported in four days last week. Notice the sharp uphill climb? That’s the story the press has been telling.
But those deaths didn’t occur on those days. In fact, the vast majority of them occurred days, or even weeks, before. The actual date of these deaths is indicated by the orange bars.
In fact, as of Sunday, the biggest one-day death toll so far in the state happened back on July 16, when 114 are known to have died. And when the press was claiming that 2,013 had died in July, the actual number of known deaths was 1,847.
As we noted in this space last week, this distortion is being repeated by the media in state after state that has seen a recent spike in coronavirus cases. While deaths attributed to coronavirus have increased, the “surge” is a fiction because many of those deaths happened earlier.
This is only one of the problems with the death counts being shouted from the media rooftops.
Here again, Florida serves as a model of how to sow fear.
First there’s the missing context.
Another way to look at it is that the death rate in Florida at the moment is 273 per million residents. In New York, it’s 1,680 and in New Jersey it’s 1,785.
In other words, the current situation in Florida is nothing at all like what happened in the northeast in the spring. Yet that critical information never gets conveyed by the press.
Another bit of missing context is where these deaths are occurring.
Of the more than 5,000 coronavirus deaths in Florida, 45% of them involved residents and staff at long-term care facilities.
That’s not to say these deaths are less important. But it does provide a needed backdrop for everyone else in the state. Their risk is tiny by comparison.
This finding also shows that what’s needed most is to protect at-risk populations, something that the generalized lockdowns failed to do. Pretending that coronavirus “doesn’t discriminate” is a dangerous fiction.
Then there’s the fact that Florida’s death count is almost certainly inflated because the state is counting people who died with the virus, not just those who died because of it.
A report by CBS-12 in West Palm Beach, for example, found that the state has counted as coronavirus deaths:
A 60-year-old man who died from a gunshot wound to the head.
A 90-year-old man who fell and died from complications of a hip fracture.
A 77-year-old woman who died of Parkinson’s disease.
Out of 581 deaths attributed to coronavirus in that county, “The I-Team found eight cases in which a person was counted as a COVID death, but did not have COVID listed as a contributing cause of death.”
What’s more, only 169 deaths were listed as due to coronavirus without any other contributing factors.
(As a side note, why is a local TV news team digging into the numbers, while the national media are content to repeat whatever the government tells them?)
As we’ve said before, this sort of overcounting is going on nationwide, largely because the CDC has told states to report deaths this way.
The question that deserves to be answered is why the mainstream press seems so willing and eager to whip up fear, rather than provide all the relevant facts, in context, so the public can make its own informed decisions about how to respond to this disease.
Professor Sunetra Gupta provides a wise, wholistic perspective on the pandemic in her interview published at Reason We may already have herd immunity. Excerpts in italics with my bolds. H/T Paul Yowell.
I particularly appreciate her sense of the complexity of multiple factors and values, and humility in the challenge of getting the balance right. This contrasts with so many narrow and overly confident technical pronouncements we read and hear in the media.
Are we already immune to coronavirus? Professor Sunetra Gupta, a theoretical epidemiologist at Oxford University, discusses her recent study on the herd immunity threshold, as well as her views on the social costs of lockdown, the inaccuracy of epidemiological models, and the curtailment of academic debate.
A study produced by a team at Oxford University indicated that some parts of the United Kingdom may already have reached herd immunity from coronavirus. A significant fraction of the population, according to the study published last week, may have “innate resistance or cross-protection from exposure to seasonal coronaviruses”, making the proportion vulnerable to coronavirus infection much smaller than previously thought.
The Oxford team is led by Sunetra Gupta, a professor of theoretical epidemiology. In recent months, she has argued that the cost of lockdown will be too high for the poorest in society and questioned the language and quality of debate on the pandemic’s impact.
Reaction interviewed Professor Gupta about these matters and more, with questions from Maggie Pagano, Alastair Benn and Mutaz Ahmed.
Cross-immunity Matters
Yes, exactly. The principle of protection from exposure to related viruses, and indeed any kind of pathogen, is one that we’ve known for a very long time. The very first vaccine we had, which is smallpox, was based on the idea that cowpox protects against smallpox. This idea was already there well in advance of us knowing that smallpox was a virus – and indeed in advance of germ theory having been properly established. So we knew about this cross protection even before we knew that diseases were caused by germs. It’s a very old idea.
In my own studies, beginning with malaria and then later thinking about flu, the role of cross-immunity in protecting against disease seemed to be something that very much needed to be factored into our thinking. Most of the people who die from malaria are children, and they die upon their first exposure, because they have no immunity at that stage. That was one of the first things that struck me when I was working on malaria.
And then later when I was working on flu, it seemed to me a very good way of explaining why the 1918 flu had killed so many people, but why that didn’t seem to be repeating itself, was that it was likely that people hadn’t been exposed to flu. Many people would have not had the flu at all. So then that built up this population of naive immunity in people under the age of thirty who were very badly affected when the pandemic came through.
Having those ideas in mind, when the Covid-19 virus started to spread, I was pretty certain it wouldn’t have a huge, devastating impact in terms of mortality, because we had all these other coronaviruses circulating.
What I didn’t anticipate was that some of our responses to previous exposure to seasonal coronaviruses might actually protect us from infection. It’s one thing to get infected and not ill, but what the new studies are showing is that people are actually fighting off infection. So at an even more basic level, the pre-existing antibodies or T-cell responses against coronaviruses seem to protect against infection, not just the outcome of infection.
Low Seroprevalence May be a Good Thing
What we know is that the seropositivity rates in many parts of the world are much lower than we’d expect them to be if we assume that the epidemic has passed through and that people are resistant. If you take a very simple scenario where everyone is susceptible, you’d expect 60-70% of them to have some marker of exposure. And that is not what’s been observed.
One of the things that’s been done in reporting the seroprevalence, which is not correct, is that they’ve been homogenised. When people say only 5-6% of the UK population has been exposed, that’s not correct. I think very few people would agree that exposure rates in London are less than 20%.
The picture that we’re getting is heterogeneous. But even in hotspots, apart from a few reports, they’re still quite low. So why is that?
One reason might be that lockdown stopped the spread of infection, so it was halted at a stage when, say, 20% of people were immune and the rest of the people were still susceptible to infection. Well, under those circumstances, the easing of lockdown should result in fairly rapid growth of cases. And that’s not something we’re seeing.
So we’ve got those two bits of information. The third bit, the missing piece of the puzzle, is this idea that some people are fully resistant to infection, because they just have really good defences. That could just be part of our innate immunological makeup. It’s also becoming clear that some of the people that have beaten it off have had responses to other coronaviruses which could have played a role.
The other bit of the puzzle is that some people do get infected and they make antibody responses, but those responses die very quickly. So if you’re trying to measure exposure, you won’t get the full picture. Some of the measures of seroprevalence might be underestimates.
We’ve got four pieces of the puzzle, then. If we put them all together, which is what the paper that we published on Friday does, it gives you a theoretical framework that you can use to look at how these bits connect up together.
You can see two things. You can see why the seroprevalence level might be low, and you can also infer that the level of herd immunity needed to stop the thing from exploding again is actually much lower than the figures that are currently being thrown around quite incautiously might suggest.
The fifth piece of this jigsaw could be that there is some seasonality. I suspect that in the winter it will probably come back, but hopefully only to the regions where it was kept from going by lockdown, and where the seroprevalence levels are genuinely extremely low.
We can be cautiously hopeful that in areas where the seroprevalence levels have achieved a certain value that’s compatible with there being a proportion who are resistant, that it might not come back with such vehemence.
Quality of Life Matters
What’s disappointed me about the way this has been approached is it has been approached along a single axis, which, if you like, is a scientific one. Even within that context, you could argue that it’s too one-dimensional, so we’re not thinking about what’s happening with other infectious diseases or how many people are going to die of cancer.
That’s the axis of disease, but then there’s the socioeconomic axis, which has been ignored. But there’s a third, aesthetic access, which is about how we want to live our lives. We are closing ourselves off not just to the disease, but to other aspects of being human.
I think the trade-off is very extreme. Obviously the most extreme manifestation of that trade-off is the 23 million people who will be pushed below the poverty line as a result of this sledgehammer approach. The costs to the arts is I think also incredibly profound – the theatres and all other forms of performing art. But also the inherent art of living, which I think is being compromised.
Acts of kindness are being eschewed. Someone was telling me yesterday that their mother said to them “please don’t come home, you’re going to kill us”.
Carrying On with Living is Social Responsibility
Because actually, the only way we can reduce the risk to the vulnerable people in the population is, for those of us who are able to acquire herd immunity, to do that.
Even if there is a little bit of a risk. I’m 55 years old, there’s some slight risk out there. But I would be willing to take that, just as I do with the flu. There’s a risk I might die of flu, but I’m willing to take that risk, because I know that if I don’t then flu will appear as it did before, it will enter the population of immunologically naive individuals, and then there will be a high risk of infection which will have a disproportionate effect on the vulnerable sector of the population.
Maybe the way to counter it now is to say, actually, not only is it a good thing for young people to go out there and become immune, but that is almost their duty. It’s a way of living with this virus. It’s how we live with other viruses. Flu is clearly a very dangerous virus, but the reason we don’t see more deaths from flu every year is because, through herd immunity, the levels of infection are kept to as low a level as we can get.
The truth is that herd immunity is a way of preventing vulnerable people from dying. It is achieved at the expense of some people dying, and we can stop that by preventing the vulnerable class in the process. In an ideal situation, you would protect the vulnerable as best you can, let people go about their business, allow herd immunity to build up, make sure the economy doesn’t crash, make sure the arts are preserved, and make sure qualities of kindness and tolerance remain in place.
We live, it seems, in this state of terror. Yes, international travel facilitates the entrance of contagion, but what it also does is it brings immunity.
Good Thing It’s Not Our First Coronavirus
If coronavirus had arrived in a setting where we had no coronavirus exposure before, we might be much worse off. It also seems that in addition to protection against severe disease as a result of exposure to related coronaviruses, some fraction of us seem to be resistant to infection.
That’s just fantastic news, actually. Hopefully that will be consolidated at a scientific, laboratory level. We ourselves are looking at how antibodies to seasonal coronaviruses can impact on protection against infection and disease.
Maybe we will be able to build up a picture that will reassure the public that actually we are much better off having been exposed to related coronaviruses. We are in a better place to fight off this infection than we actually thought.
Abstract It is widely believed that the herd immunity threshold (HIT) required to prevent a resurgence of SARS-CoV-2 is in excess of 50% for any epidemiological setting. Here, we demonstrate that HIT may be greatly reduced if a fraction of the population is unable to transmit the virus due to innate resistance or cross-protection from exposure to seasonal coronaviruses. The drop in HIT is proportional to the fraction of the population resistant only when that fraction is effectively segregated from the general population; however, when mixing is random, the drop in HIT is more precipitous. Significant reductions in expected mortality can also be observed in settings where a fraction of the population is resistant to infection. These results help to explain the large degree of regional variation observed in seroprevalence and cumulative deaths and suggest that sufficient herd-immunity may already be in place to substantially mitigate a potential second wave.
Initial results indicate fewer than 1 in 100 blood donations have antibodies to the novel coronavirus that causes COVID-19.
The header emphasizes how few blood samples showed antibodies, while the more important finding about reduced lethality of Covid19 requires searching in the fine print.
Context
Today, Canadian Blood Services and Canada’s COVID-19 Immunity Task Force (CITF) are releasing initial results of the first 10,000 blood donor samples assessed for SARS-CoV-2 antibodies. This analysis reveals that over the period May 9 through June 8, 2020, fewer than 1 per cent of the 10,000 samples from blood donors tested positive for antibodies to the novel coronavirus. Antibodies indicate past infection with SARS-CoV-2, and population studies like this one tell us how many people have likely been exposed to the virus.
These results offer a first, high-level glimpse into an ongoing Canadian Blood Services study assessing SARS-CoV-2 antibodies across nine provinces. They will be updated once Canadian Blood Services completes their analysis of the full sample of 37,800 donations made during the months of May and June 2020. In addition, Héma-Québec will have results for Quebec in the near future, which will be important for a complete national picture, given the COVID-19 rates in that province.
“What is clear is that only a small percentage of adult Canadians has been infected by SARS-CoV-2,” Hankins says. “By far, the majority of us remain vulnerable to infection. We need to ramp up testing and tracing capacity across the country to interrupt any chains of transmission quickly to prevent unchecked spread.”
Acknowledging that many more adult Canadians are infected than currently documented, Professor Timothy Evans, CITF Executive Director cautioned against over-interpreting the apparent reduction in risk. “Among adults, the death rate from being infected with SARS-CoV-2 is likely closer to one per cent, as compared to the eight per cent reported to date among those diagnosed with COVID-19. But this is a highly infective virus that could take a huge toll if we allow it to spread, and we are only now learning that many survivors have persistent symptoms.”
B.C. Centre for Disease Control research also suggests province’s true infection rate is about eight times the rate based on reported cases
The study is the first in Canada to report infection rates based on seroprevalence, which is a measure of the presence in blood samples of antibodies produced to resist the virus. Determining exactly how many people in Canada have been exposed to COVID-19 is a key goal of the immunity task force the federal government set up in April.
Timothy Evans, a member of the task force and director of McGill University’s school of population and global health in Montreal, said the B.C. survey indicates the province’s deft management of the first wave of the pandemic resulted in very low exposure across its population.
“The low prevalence of population immunity suggests that continued vigilance and adherence to best practices to reduce risk of infection will be critical, especially in the context of the second wave of the pandemic,” Dr. Evans said.
He added that the eight-to-one ratio of actual to reported cases is consistent with international studies and that he expected a similar result across Canada. The survey was based on blood samples from more than 1,700 people in two periods, one in mid-March and a second in late May. The data were gathered anonymously from residual blood drawn from individuals at diagnostic clinics in B.C.’s Lower Mainland. The subjects were males and females of varying ages, including children.
Dr. Jha, who is leading a seroprevalence study that aims to sample as many as 10,000 Canadians, also said the individuals in the B.C. study may not be representative of the province’s population. For example, the study may be skewed toward healthy people who were having their blood tested as a precaution, or by those who were already ill.
It also captured the presence of antibodies in blood samples before and after the first wave but not during the peak in April. Another key piece of information the B.C. study does not provide – and was not designed to – is whether the individuals found to have antibodies for COVID-19 are now immune to the coronavirus and, if so, for how long.
My Comment:
Up to now, we have only been able to estimate the lethality of Covid19 by comparing death rates to confirmed cases. In Canada as of July 17, 2020, there were 8839 deaths of people with Covid19 compared to 109669 confirmed cases, or 8.1%. If the actual # of infections was 8 times higher, that ratio drops to 1% lethality. Furthermore, the ratio of deaths/cases ranged as high as 14% early June, and is now down to 3%. Factoring in the hidden infections reduces the current lethality to 0.4%.
Of course this is preliminary reporting while we await results from the nation-wide study. I do object to the “second wave” narrative parroted in the media to keep the fears alive. Also the public is never presented the big picture about national mortality.
Canada Pop
Ann Deaths
Daily Deaths
Risk per Person
2019
37589262
330786
906
0.8800%
Covid 2020
37589262
8839
60
0.0235%
Over the epidemic months, the average Covid daily death rate amounted to 7% of the All Causes death rate. During this time a Canadian had an average risk of 1 in 5000 of dying with SARS CV2 versus a 1 in 114 chance of dying regardless of that infection. As shown later below the risk varied greatly with age, much lower for younger, healthier people. Presently daily Covid deaths are hovering around 10, or 1% of deaths from all causes.
B.C. Centre for Disease Control research also suggests province’s true infection rate is about eight times the rate based on reported cases
The study is the first in Canada to report infection rates based on seroprevalence, which is a measure of the presence in blood samples of antibodies produced to resist the virus. Determining exactly how many people in Canada have been exposed to COVID-19 is a key goal of the immunity task force the federal government set up in April.
Timothy Evans, a member of the task force and director of McGill University’s school of population and global health in Montreal, said the B.C. survey indicates the province’s deft management of the first wave of the pandemic resulted in very low exposure across its population.
“The low prevalence of population immunity suggests that continued vigilance and adherence to best practices to reduce risk of infection will be critical, especially in the context of the second wave of the pandemic,” Dr. Evans said.
He added that the eight-to-one ratio of actual to reported cases is consistent with international studies and that he expected a similar result across Canada. The survey was based on blood samples from more than 1,700 people in two periods, one in mid-March and a second in late May. The data were gathered anonymously from residual blood drawn from individuals at diagnostic clinics in B.C.’s Lower Mainland. The subjects were males and females of varying ages, including children.
Dr. Jha, who is leading a seroprevalence study that aims to sample as many as 10,000 Canadians, also said the individuals in the B.C. study may not be representative of the province’s population. For example, the study may be skewed toward healthy people who were having their blood tested as a precaution, or by those who were already ill.
It also captured the presence of antibodies in blood samples before and after the first wave but not during the peak in April. Another key piece of information the B.C. study does not provide – and was not designed to – is whether the individuals found to have antibodies for COVID-19 are now immune to the coronavirus and, if so, for how long.
My Comment:
Up to now, we have only been able to estimate the lethality of Covid19 by comparing death rates to confirmed cases. In Canada as of July 17, 2020, there were 8839 deaths of people with Covid19 compared to 109669 confirmed cases, or 8.1%. If the actual # of infections was 8 times higher, that ratio drops to 1% lethality. Furthermore, the ratio of deaths/cases ranged as high as 14% early June, and is now down to 3%. Factoring in the hidden infections reduces the current lethality to 0.4%.
Of course this is preliminary reporting while we await results from the nation-wide study. I do object to the “second wave” narrative parroted in the media to keep the fears alive. Also the public is never presented the big picture about national mortality.
Canada Pop
Ann Deaths
Daily Deaths
Risk per Person
2019
37589262
330786
906
0.8800%
Covid 2020
37589262
8839
60
0.0235%
Over the epidemic months, the average Covid daily death rate amounted to 7% of the All Causes death rate. During this time a Canadian had an average risk of 1 in 5000 of dying with SARS CV2 versus a 1 in 114 chance of dying regardless of that infection. As shown later below the risk varied greatly with age, much lower for younger, healthier people. Presently daily Covid deaths are hovering around 10, or 1% of deaths from all causes.
Coordinator of the Integrated Toxicological Surveillance Center (Civitox), the toxicologist and nutritionist Sandro Benites is an advocate for the use of the Covid Kit, which includes drugs such as Hydroxychloroquine, Azithromycin, Ivermectin, Zinc and Vitamin D for early treatment of Covid-19.
In Campo Grande he led a group of 300 doctors who convinced Mayor Marquinhos Trad to adopt the service protocol that includes the distribution of the kit, with medical prescription in specific cases. The same protocol was adopted in 12 other Brazilian capitals and is being studied in the others. It was developed based on experiences that worked in countries like Spain and the United States, even before the pandemic reached Brazil, according to the doctor.
In an interview with O PROGRESSO, he was categorical in stating that these drugs are effective in early treatment and do not bring health data, as long as used following medical guidelines.
Read the interview here:
Q: Mayor Marquinhos Trad recently adopted the protocol proposed by you and a group of 300 doctors, which provides for the distribution of Kits against Covid-19. In practice, what changes from now on?
A: What changes is that several doctors were doing this initially in the office very successfully while others did not because they had a hard time supporting themselves. Today this group has the support and the release of the CRM (Regional Council of Medicine), the Medical Association of Mato Grosso do Sul, the Brazilian Medical Association and the Union of Doctors, in other words, it is easier for several colleagues to join. It is one thing for a doctor to act in isolation, another thing for a group of doctors to adopt this protocol together with the highest authority in the municipality, which in the case of Campo Grande is Mayor Marquinhos Trad.
Q: What is the purpose of this protocol?
A: Our goal is to make the population see that they cannot be isolated inside the home with symptoms. What society needs to understand is that a patient who arrives with fever, malaise or a cough, needs to be seen. He must have an x-ray, a blood count and be treated. The medical profession, which until then was acting in a way, needs to rethink this attitude of only attending or interning only if the patient is in a serious situation or with shortness of breath. From now on, like everything in medicine, if you start treatment early, the chance of success is greater. In this way, prevention is simpler, more efficient, more effective and cheaper.
Q: Do these drugs cure the disease?
A: There is no cure for the disease. It is a virus that is not even considered a living being.
These medications are intended to inhibit viral replication within the cell and the disease does not worsen, thus preventing the patient from having to go to an ICU tube, for example. The result of this is that we reduce this chaos that we are experiencing due to the lack of structure in hospitals.
Q: As you evaluate the current protocol used in most of the country, to diagnose the patient and not medicate, just send him to stay at home in isolation. Is that a risk?
A: This is a huge risk. Today the patient who has a headache, malaise and coughing goes home to take dipyrone. I prefer to take hydroxychloroquine. It is a safe medication that we have used in medical practice for over 80 years. I have worked in an intoxication center here in the State for almost 20 years and I have never seen hydroxychloroquine or ivermectin intoxication.
The same happens in other centers in Brazil. As a major in the Brazilian Army, I know that all military personnel in the Armed Forces, whether Navy, Army or Air Force, when the transfer to the Amazon region takes place_ and hundreds of families have been transferred for decades_ they use hydroxychlorquine or even chloroquine. And what risk do they have? None.
Q:How do you evaluate the deaths that occurred in Manaus due to the use of the medication?
A: There was work in Manaus, which in my view is something worthy of a crime.
Toxic doses were given to patients, up to five times more than the therapeutic dose, leading to the death of these people.
This group of scientists proved that when a lethal dose is given to a patient, lethality happens. This fact confused society. The doctor is part of society and when he sees this there, he is not used to using these drugs and this failure ends up happening. The result of this was that we ended up wasting a lot of time and certainly a lot of lives.
Q: What is the profile of the patient who will receive the medication and in what way?
A: It is not for everyone to use. There is no medicine for 200 million inhabitants. Who should use the medication are the professionals in the risk area, who are on the front line of Covid-19, working in CTI, Emergency Room, hospital or UPA. These need to be paid preventively. Another audience that also needs to be medicated is that of people who had contact with someone who had Covid-19 and developed the disease. If your wife, son, father, or mother, for example, developed the disease, you need to take the medication to keep from developing too. I’m talking about the use of Ivermectin, hydroxychloroquine used in a preventive way. However, we are not talking about a medication protocol, since there is no miracle drug. We are talking about a care protocol, which provides, for example, what to be used in phase 1 of the disease, in phase 2a, in phase 2b and in phase 3, for example. The disease has several stages and each medication must be used by the doctor, with a medical prescription. There is no use going out desperate to buy medication, using an unnecessary way. This means that those who really need it end up not having access.
Q: Why is there still no scientific evidence for the effectiveness of these drugs in the case of Covid-19?
A: It is necessary to understand that there are the types of scientific evidence, scientific evidence and scientific evidence required by medical societies. Medical societies, where you find a doctor with a doctorate, post-doctorate, demand in peacetime, that you have to have scientific proof, that is, it takes months and years for a medication to be considered level A, B or C of evidence scientific. These are steps that cannot be skipped. It is logical that there is no scientific evidence of the way that some political and health authorities want. It is an insane thing for you to require scientific proof for nothing. What I’ll do? I’m going to let the patient run low, fold your arms and say you have no proof? Likewise, there is no evidence that if you intubate a patient with Covid-19 he will survive, so why am I not intubating him? There is no scientific evidence for this disease for practically nothing because the treatment framework for Covid-19 is empty.
Someone needs to be bold enough to go there to complement this picture. Either I start to put some medications or I leave the board empty. Bureaucratic medicine loses ground in times of war and in times of pandemic. No living doctor experienced a pandemic 100 years ago. So you need flexibility, boldness, humility, let go of pride and vanity, acknowledge mistakes, start over and that is not easy. Now if you think about the good of the population and the lives that can be saved, this task becomes easier. Look at the privilege we are having! A wonderful geographical privilege! We had this pandemic beginning in Asia, back in China, went to Oceania, Europe, North America and finally arrived here in South America. Many doctors in the world had positive and negative experiences without having time to publish a scientific article in indexed magazine.
This privilege is wonderful because we can see who had a positive result and copy it here. If a Brazilian doctor, Marina Bucar, presented a series of positive results back in Spain, with the same protocol that we have implemented here in Campo Grande, will I refuse to do it and cross my arms?
If the Jewish doctor, Dr. Vlademir Zelenko in New York saved more than 500 people with this protocol, will I say no? Will I wait for the scientific journal? There is no time because the hospitals are getting crowded.
Campo Grande is even more privileged because we are in the middle of the country, since this epidemic first arrived in São Paulo, the financial capital of the country, went to the administrative capital: Brasília, followed to the capital of Tourism: Rio de Janeiro and Manaus , for example. So doctors in those locations had to take action. In Belém do Pará, for example,Unimed made this protocol that we are implementing in Campo Grande when what we call the Health collapse was happening, which is when hospitals close their doors. People were unable to enter hospitals because it was padlocked. They died at the unit’s door. Do we want this for our city? No. When that happened in Belem they adopted this protocol and within a week they solved the problem. If this is not scientific evidence, for me, nothing else will be.
Porto Feliz, in São Paulo, adopted the same measure, that is, more action and less bureaucracy since we have no time to lose.
Q: Are these drugs bad for your health?
A: People are afraid of the possible side effect of the medication. I do not. I’m afraid of the effect of the virus, Covid-19. Let’s say that if I have to take the medication for five days and on the third day I have side effects, what do I do? I stop taking it, just that. The medication is not going to kill me. If I take it and give me diarrhea or vomit I stop. There are people who can’t take contraceptives, others can’t take Dipirona, it’s simple.
Q: Why is there so much resistance on the part of governments to adopt the use of these drugs as a protocol?
A: Do not know. Because it is useless to use rational arguments for something irrational not to adopt the service protocol. If I say that no Intoxication Center has registered the death of someone from the use of these drugs over the age of 35, it is a rational argument. If I say that all military personnel receive hydroxychloroquine and none have died over the past 50 years, it is a rational argument. If I say that the people who have it is lupus, psoriasis they use for years is a rational argument. If I say that if the person has any side effects, just suspend the use, it is a rational argument. So there is no point in using rational arguments for something that is irrational, that I cannot understand.
Q: What are the risks that municipalities like Dourados run in not adopting this protocol?
A; Losing lives that could be saved.
Q:What motivated you to oppose a good part of the medical profession and defend the use of this protocol?
A: What motivated me was the fact that I see that I do not need an indexed scientific journal to take my course, in addition to perceiving other colleagues successfully, listening and having this flexibility and having the courage to do it here in Campo Grande.
I think the moment is not one of nitpicking, but of union. This is not the time for us to be divided. Doctors, population, managers, in short, everyone will benefit from it: managers for saving lives, doctors feeling fulfilled in their profession and the population losing their morbid fear of this virus, knowing that there is an effective treatment. We need to stop this political issue.
My fear cannot be greater than my responsibility as a doctor. It is unthinkable for a health professional to want scientific evidence at the time of tragedy. Medicine has never grown so much in major world wars or pandemics because bureaucrats are losing space. It is time for doctors of action and daring to act. So I think we are blessed, let’s put everything aside and let’s think more about our population. It’s very simple, the people who complicate it. When human beings want to complicate, they complicate.
From Dr. George Fareed’s letter to President Trump and the Task Force:
In my attempts to keep people alive, I have had an opportunity to use many different types of treatments — remdesivir, dexamethasone, convalescent plasma replacement, etc. Yet, by far the best tool beyond supportive care with oxygen has been the combination of hydroxychloroquine (HCQ), with either azithromycin or doxycycline, and zinc. This “HCQ cocktail” (that costs less than $100) has enabled me to prevent patients from being admitted to the hospital, as well as help those patients that are hospitalized.
The key is giving the HCQ cocktail early, within the first five days of the disease.
Not only have I seen outstanding results with this approach, I have not seen any patient exhibit serious side-effects. To be clear — this drug has been used as an anti-malarial and to treat systemic lupus erythematosus as well as rheumatoid arthritis, and has over a 50-year track record for safety. It is shocking that it only now is being characterized as a dangerous drug.
Moreover, I am in my seventies, and I (as well as some other older physicians in the hospital) use hydroxychloroquine and zinc as prophylaxis. None of us have contracted the disease despite our high exposure to COVID patients nor have we experienced any side-effects.
Despite the characterization in the mainstream media as the drug being “ineffective” and “dangerous,” the evidence in the literature tells a different story. I am not only an “MD,” but a former Harvard Medical School assistant professor and UCLA School of Medicine associate professor as well and am very competent at evaluating studies.
There is ample evidence now that the HCQ cocktail is effective and there is no good evidence that there are significant side effects.
I am writing to you out of the frustration of knowing that there is a solution, but watching as our country flounders in dealing with COVID-19. In my opinion, tens of thousands are dying unnecessarily. Our current approach of waiting for these high-risk patients to become ill and then hospitalizing them is failing. The answer is early diagnosis of the high-risk individuals, and then treating them as outpatients with the HCQ cocktail to prevent hospitalization.
So, what I am proposing is a drastic shift from our current approach: we need to ramp up our outpatient efforts of treating COVID-19 to decrease the burden on hospitals and save lives.
Such an approach requires an effective outpatient treatment — we have that in the HCQ cocktail.
By analyzing the Portuguese anonymized data on private and public based medical prescriptions we have identified all cases chronically receiving HCQ for the management of diseases such as systemic lupus erythematosus, rheumatoid arthritis, and other autoimmune diseases. Additionally, we have detected all laboratory confirmed cases of SARS-CoV-2 infection and all laboratory confirmed negative cases in the Portuguese population (mandatorily registered in a centrally managed database). Cross linking the two sets of data has allowed us to compare the proportion of HCQ chronic treatment (at least 2 grams per month) in laboratory confirmed cases of SARS-CoV-2 infection with laboratory confirmed negative cases.
Results: Out of 26,815 SARS-CoV-2 positive patients, 77 (0.29%) were chronically treated with HCQ, while 1,215 (0.36%) out of 333,489 negative patients were receiving it chronically (P=0.04). After adjustment for age, sex, and chronic treatment with corticosteroids and/or immunosuppressants, the odds ratio of SARS-CoV-2 infection for chronic treatment with HCQ has been 0.51 (0.37-0.70).
Conclusions: Our data suggest that chronic treatment with HCQ confers protection against SARS-CoV-2 infection.
This overheated US election cycle is turbocharged with Pandemania, with viral fear weaponized for political advantage. In this context Texas provides a window into the struggle between reason and panic regarding data gathered to inform the public on the spread of this contagion. An example is this recent inflammatory article at partisan The Daily Beast TexasErases COVID Cases—and Fans Conspiracy Theory Flames. Excerpts in italics with my bolds.
When health officials quietly removed nearly 3,500 COVID-19 cases from the official Texas total on Wednesday, it launched a deluge of conspiracy theories about inflated and unreliable data in the midst of a surging pandemic.
The 3,484 removed cases were diagnosed using FDA-approved antigen tests. The FDA has said positive results from antigen tests are “highly accurate,” and can be used to diagnose current COVID-19 infections. But state health officials pointed to the definition of a coronavirus case the CDC published in early April to explain why the cases were removed.
“The case data on our website reflect confirmed cases, and cases identified by antigen testing are considered probable cases under the national case definition,” said Chris Van Deusen, a spokesman for the Texas Department of State Health Services.
Under that definition, the CDC only considers cases “confirmed” if they are diagnosed using a molecular, often called PCR, test. Cases that are detected using antigen tests are classified as “probable.” If someone is diagnosed with an antigen test, Texas will not count their case among the state total.
Texas will now separate viral and antibody tests before calculating positivity rating
With antibody testing on the rise, Texas is changing the way it reports the positivity rating — the percentage representing the number of people who have tested positive for COVID-19 over a given period of time.
The positivity rating is one of a number of metrics used by state officials when they determined how to reopen the state amid the pandemic. In early to mid-April, numbers from the Texas Department of State Health Services showed positivity ratings in Texas were well over 10%.
When Gov. Greg Abbott announced his Open Texas plan in late April, the positivity rating had dropped to about 6%, and he cautioned that should the rating again climb to a sustained trend of around 10% that it would be a “red flag” that state leaders would have to look at.
Now, as the Open Texas plan rolls on, more attention is being given to the rating as an indicator of the continued spread of the 2019 novel coronavirus. Texas, as it turns out, is one of at least four states, including Vermont, Virginia and Georgia, that are combining numbers from two different tests, viral and antibody, to calculate the positivity rating.
Viral tests, performed through a nose or saliva swab, determine if a person is currently fighting the virus.Antibody tests, performed by a blood sample, look for signs a person has been exposed to the virus in the past but are not currently infected.
Some experts said combining the two can provide a misleading picture of the current spread of the virus and overstates the ability to test and track infections, a key consideration as the state eases restrictions put in place to curb the spread of the virus.
Comment: There is already an equivocation fallacy in labeling someone testing positive for SARS CV2 as a case of the Covid19 disease. In the absence of illness, there is only an infection defeated by a person’s immune system. Now they want to inflate case numbers with people who were infected in the past without needing treatment. Those people are better deemed “recoveries” than “cases”, and should in no way be added to the case count.
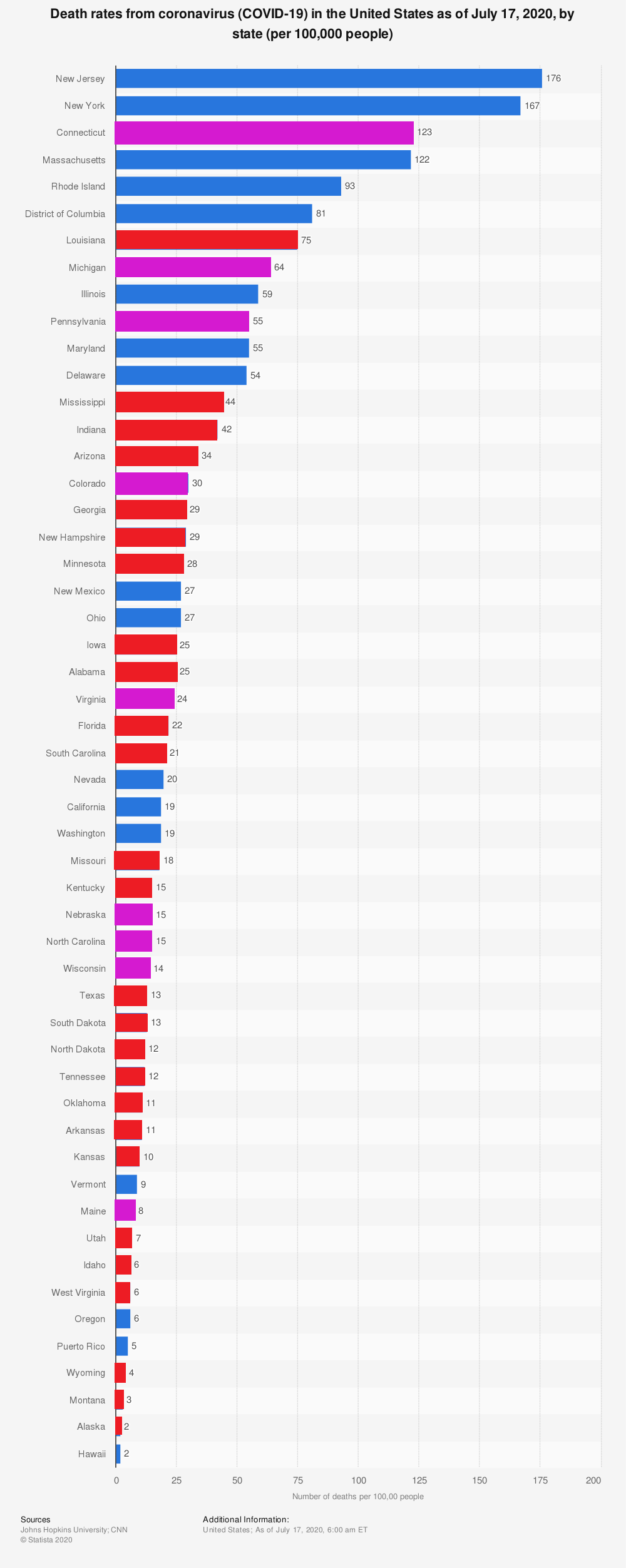
The Politics driving partisans like those at the Beast are suggested by the graph below.
I have colored Blue the states controlled by the Democrat party, Red for Republican strongholds, and Purple for the battleground states. I did mostly follow the partisan state designations in Wikipedia, though obviously, there is some subjectivity in these evaluations. For example, Louisiana is traditionally Red, but the current Governor is Democrat John Bel Edwards. And Minnesota appears Red but is governed by a Democrat. The problem for Democrats seeking to take power by stoking Covid fears is that they are governing the states with the highest death rates. NY and NJ have death rates well over 100 per 100,000, while Florida counts 22 and Texas sits at 13. For some reason, west coast Blue states have fared better. But Texas with its large number of electoral delegates is the political prize, hence the media trickery.
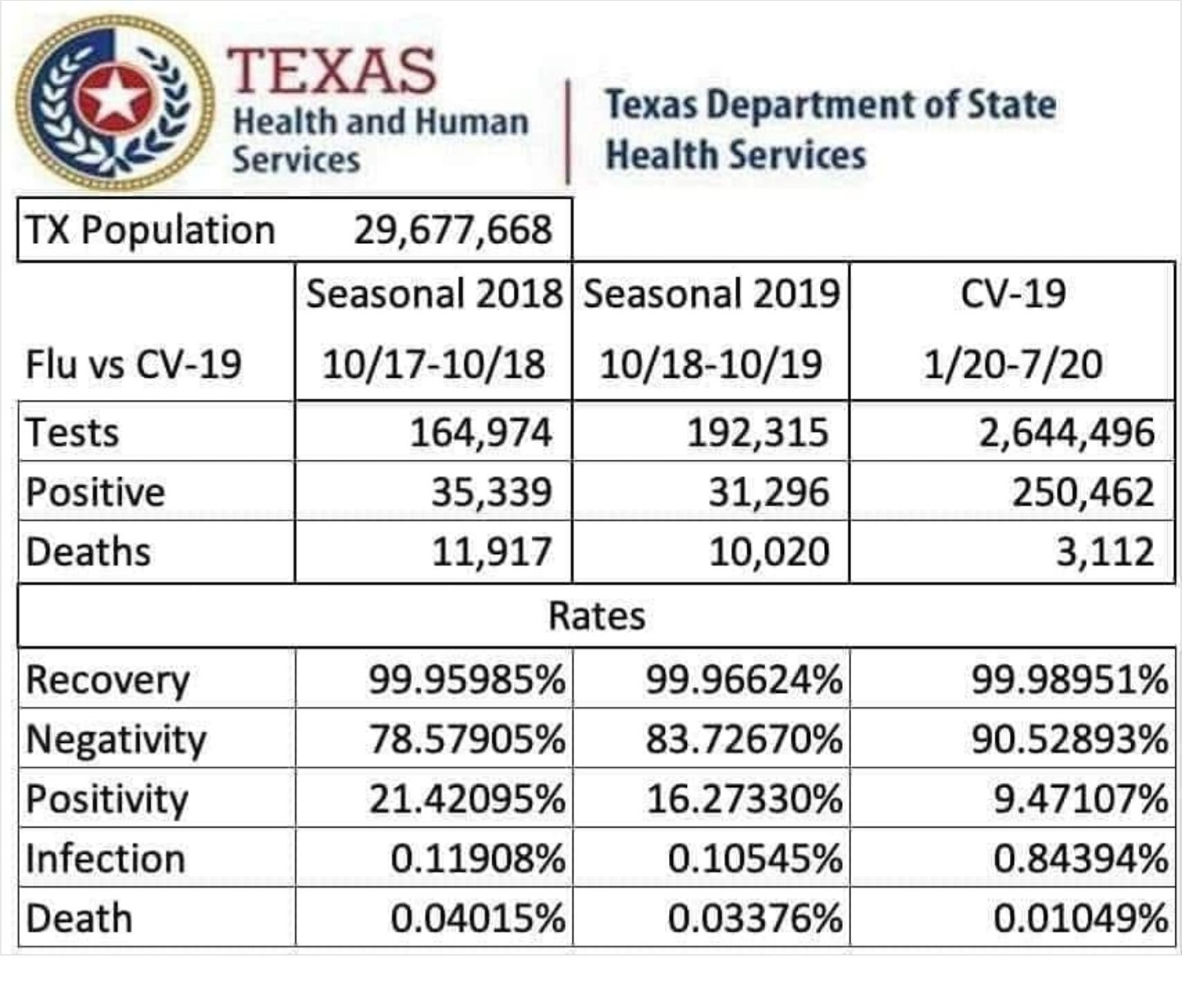
Some controversy was created when a doctor compiled this graphic:
Those wanting not to moderate fears but to amplify panic objected that the chart was not produced by DSHS, and Covid should not be compared to the flu. But a more detailed comparison confirms what the chart suggests. Doing the math to keep things in proportion.
First Covid death in Texas was on March 23, 2020. 16 weeks later total deaths 3506, or 219 reported Covid19 deaths a week. If that rate continue another 36 weeks ( a big if), Texas would report 11, 394 deaths, comparable to a typical flu year. If Texas gets this back under control like it was pre-July, the number will be lower than a flu year. If not, the total could climb higher. The present spike in positive tests started July 8, and officials are determined to rein it in, but we shall have to wait and see.
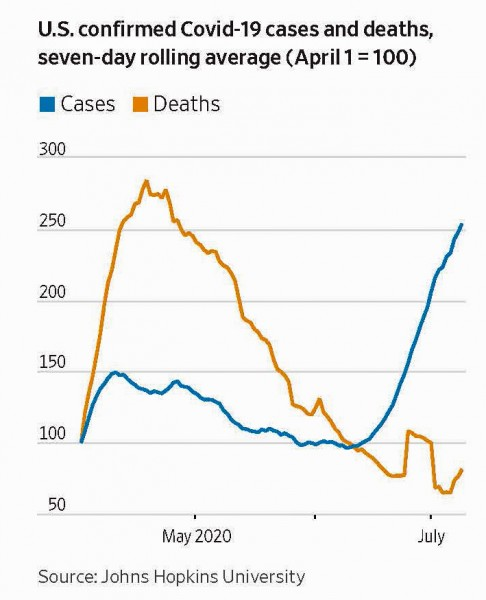
The overall US picture is not discouraging, since more cases have not stopped the decline in deaths:
The map shows that in Canada 8839 deaths have been attributed to Covid19, meaning people who died having tested positive for SARS CV2 virus. This number accumulated over a period of 148 days starting January 31. The daily death rate reached a peak of 177 on May 6, 2020, and is down to 11 as of yesterday. More details on this below, but first the summary picture. (Note: 2019 is the latest demographic report)
Canada Pop
Ann Deaths
Daily Deaths
Risk per Person
2019
37589262
330786
906
0.8800%
Covid 2020
37589262
8839
60
0.0235%
Over the epidemic months, the average Covid daily death rate amounted to 7% of the All Causes death rate. During this time a Canadian had an average risk of 1 in 5000 of dying with SARS CV2 versus a 1 in 114 chance of dying regardless of that infection. As shown later below the risk varied greatly with age, much lower for younger, healthier people.
The Key Covid Metric
With easing of lockdowns and increased testing in many places, epidemiologists are focusing on a key metric to inform public policies: Positivity. The positivity metric is the rate (%) of people who test positive out all people sampled. The significance is that (by definition) a presumed case is a person who tests positive once. If a second test comes back positive it is a confirmed case. The metric is not perfect for two reasons.
The first problem is false positives from the testing procedure itself or from errors in the data processing and reporting. For this we have to hope that quality assurance protocols are being followed and mistakes corrected along the way.
The larger issue appeared in Florida recently when officials discovered that numerous batches of samples were reported 100% positive and other batches 100% negative. While the latter result is expected sometimes, all people testing positive seems unlikely. Behind this is the reality that in many situations (eg hospital ICU) a single patient will be tested many times with many positive results in the course of monitoring that individual’s clearing of the virus. Obviously a batch of samples from that ICU might legitimately be 100% positive.
But it is also true that 10 or 20 positive tests from one patient should not be reported as 10 or 20 new cases. In some jurisdictions, officials say they go to the effort to link test results to the individuals tested, and can distinguish between number of cases and number of positives. In other places, cases and positives may be the same number. Thus confirmed cases could be only 1/2 of the total positives, or less.
How is Canada Doing?
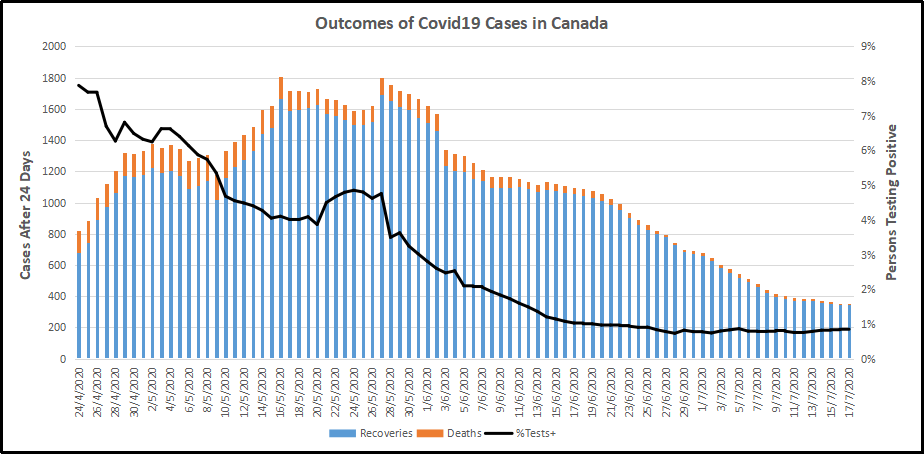
Recoveries are calculated as cases minus deaths with a lag of 24 days. Daily cases and deaths are averages of the seven days ending on the stated date. Recoveries are # of cases from 24 days earlier minus # of daily deaths on the stated date. Since both testing and reports of Covid deaths were sketchy in the beginning, this graph begins with daily deaths as of April 24, 2020 compared to cases reported on March 31, 2020.
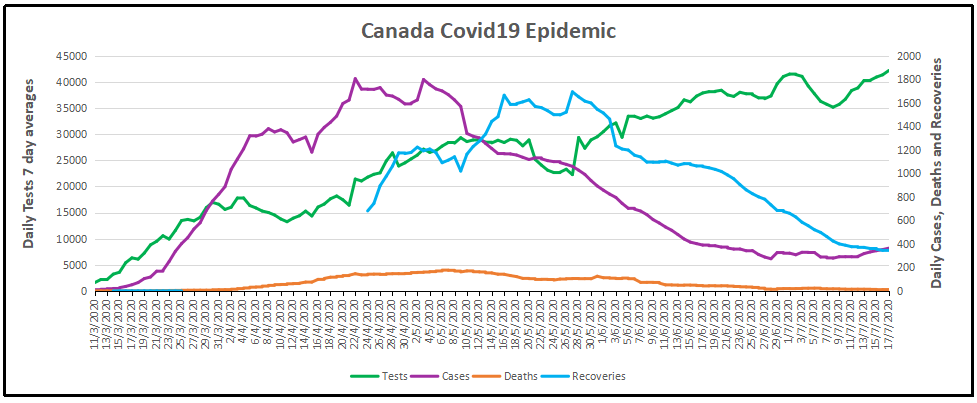
The line shows the Positivity metric for Canada starting at nearly 8% for new cases April 24, 2020. That is, for the 7 day period ending April 24, there were a daily average of 21,772 tests and 1715 new cases reported. Since then the rate of new cases has dropped down, now holding steady at ~1% for the last month. Yesterday, the daily average number of tests was 42,191 with 363 new cases. So despite double the testing, the positivity rate is not climbing.
Another view of the data is shown below.
The scale of testing has increased and is now exceeding 40,000 a day, while positive tests (cases) dwindled to 1%. The shape of the recovery curve resembles the case curve lagged by 24 days, since death rates are a small portion of cases. The recovery rate has grown from 83% to 97% steady over the last 3 weeks. This approximation surely understates the number of those infected with SAR CV2 who are healthy afterwards, since antibody studies show infection rates multiples higher than confirmed positive tests. In absolute terms, cases are now down to 363 a day and deaths 11 a day, while estimates of recoveries are 345 a day.
Note: We are expecting an initial report from the National Immunity Task Force any day now regarding a major program of testing random blood samples for SARS CV2 anti-bodies.
Aside: While preparing this post I was watching CBC channel, and the scroll bar had the text: Canada passes 100,000 Covid cases. I thought, what was the point of that? Then I realized:
My bad. That is the Health Minister of PEI solemnly announcing in July their first Covid case in two months.
Background Updated from Previous Post
In reporting on Covid19 pandemic, governments have provided information intended to frighten the public into compliance with orders constraining freedom of movement and activity. For example, the above map of the Canadian experience is all cumulative, and the curve will continue upward as long as cases can be found and deaths attributed. As shown above, we can work around this myopia by calculating the daily differentials, and then averaging newly reported cases and deaths by seven days to smooth out lumps in the data processing by institutions.
A second major deficiency is lack of reporting of recoveries, including people infected and not requiring hospitalization or, in many cases, without professional diagnosis or treatment. The only recoveries presently to be found are limited statistics on patients released from hospital. The only way to get at the scale of recoveries is to subtract deaths from cases, considering survivors to be in recovery or cured. Comparing such numbers involves the delay between infection, symptoms and death. Herein lies another issue of terminology: a positive test for the SARS CV2 virus is reported as a case of the disease COVID19. In fact, an unknown number of people have been infected without symptoms, and many with very mild discomfort.
This discussion takes the assumption that anyone reported as dying from COVD19 tested positive for the virus at some point prior. A recent article by Nic Lewis at Climate Etc. referred to evidence that the average time from infection to symptoms is 5.1 days, and from symptoms to death 18.8 days. A separate issue, of course, is that 95+% of those dying had one or more co-morbidities contributing to the patient’s demise. Setting aside the issue of dying with/from Covid19, it is reasonable to assume that 24 days after testing positive for the virus, survivors can be considered recoveries.
Previous Post May 20, 2020
It is really quite difficult to find cases and deaths broken down by age groups. For Canadian national statistics, I resorted to a report from Ontario to get the age distributions, since that province provides 69% of the cases outside of Quebec and 87% of the deaths. Applying those proportions across Canada results in this table. For Canada as a whole nation:
Age
Risk of Test +
Risk of Death
Population per 1 CV death
<20
0.05%
None
NA
20-39
0.20%
0.000%
431817
40-59
0.25%
0.002%
42273
60-79
0.20%
0.020%
4984
80+
0.76%
0.251%
398
In the worst case, if you are a Canadian aged more than 80 years, you have a 1 in 400 chance of dying from Covid19. If you are 60 to 80 years old, your odds are 1 in 5000. Younger than that, it’s only slightly higher than winning (or in this case, losing the lottery).
As noted above Quebec provides the bulk of cases and deaths in Canada, and also reports age distribution more precisely, The numbers in the table below show risks for Quebecers.
Age
Risk of Test +
Risk of Death
Population per 1 CV death
0-9 yrs
0.13%
0
NA
10-19 yrs
0.21%
0
NA
20-29 yrs
0.50%
0.000%
289,647
30-39
0.51%
0.001%
152,009
40-49 years
0.63%
0.001%
73,342
50-59 years
0.53%
0.005%
21,087
60-69 years
0.37%
0.021%
4,778
70-79 years
0.52%
0.094%
1,069
80-89
1.78%
0.469%
213
90 +
5.19%
1.608%
62
While some of the risk factors are higher in the viral hotspot of Quebec, it is still the case that under 80 years of age, your chances of dying from Covid 19 are better than 1 in 1000, and much better the younger you are.
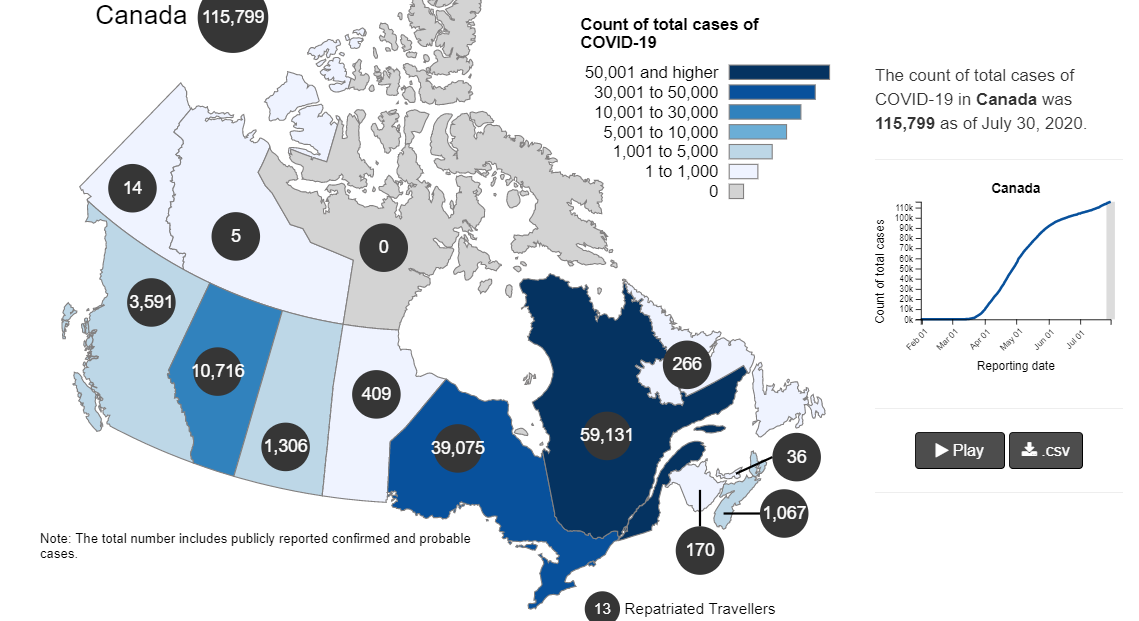
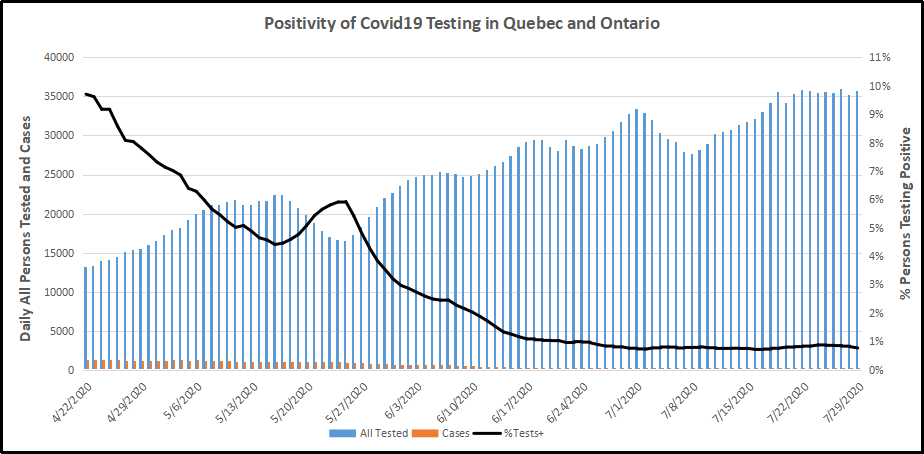
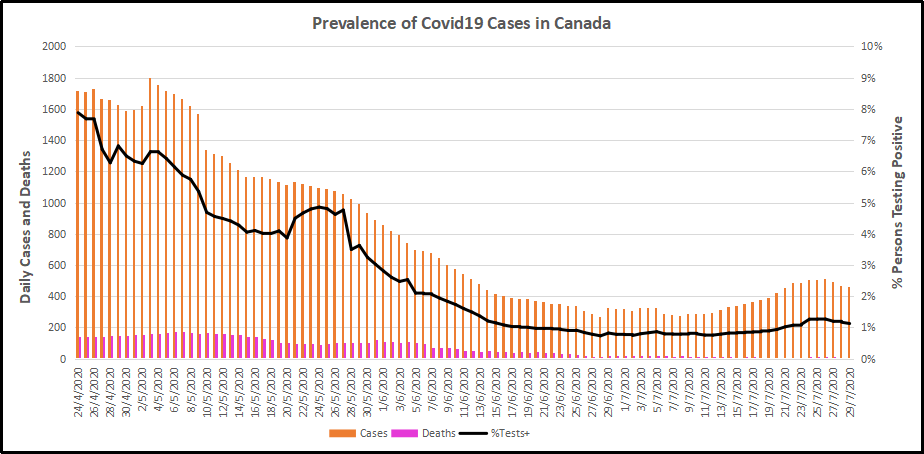


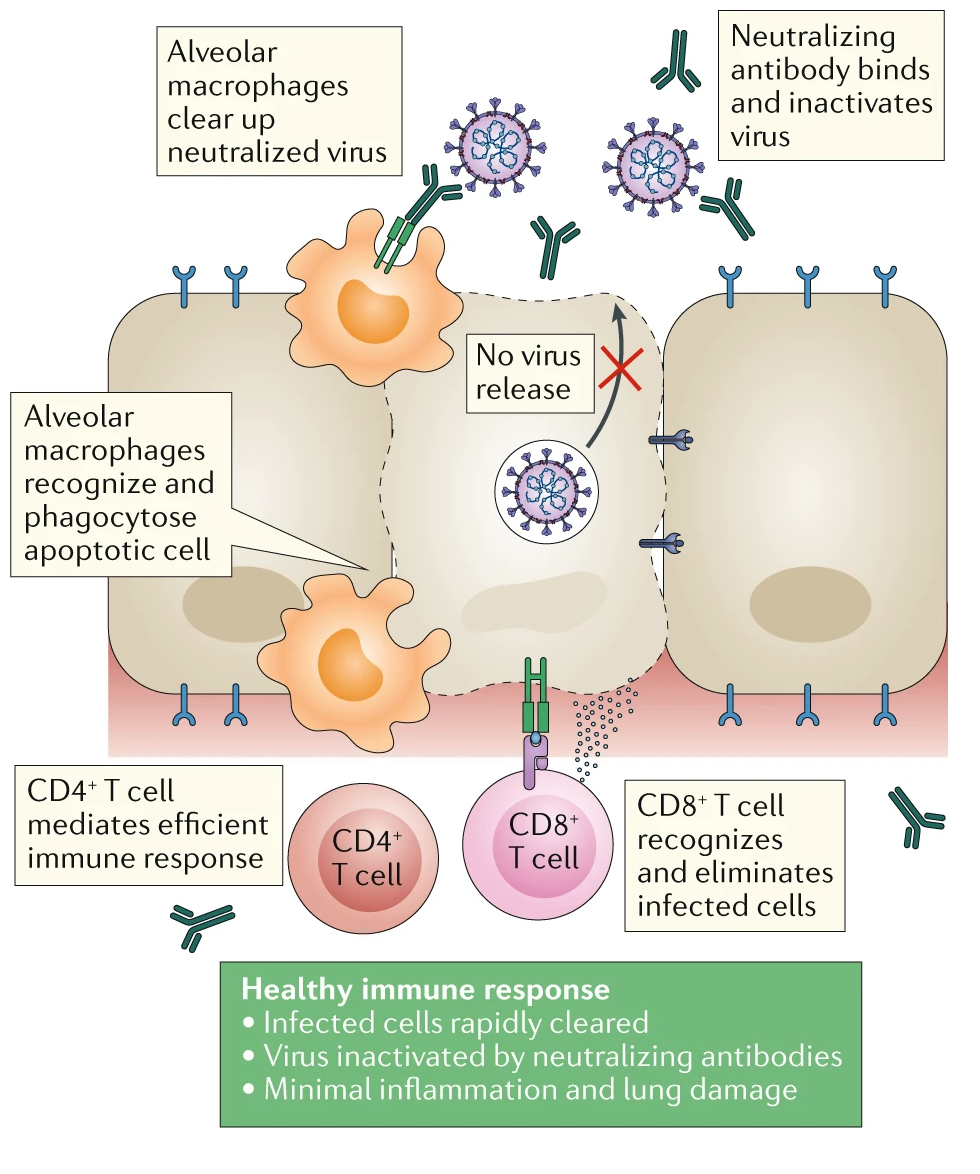





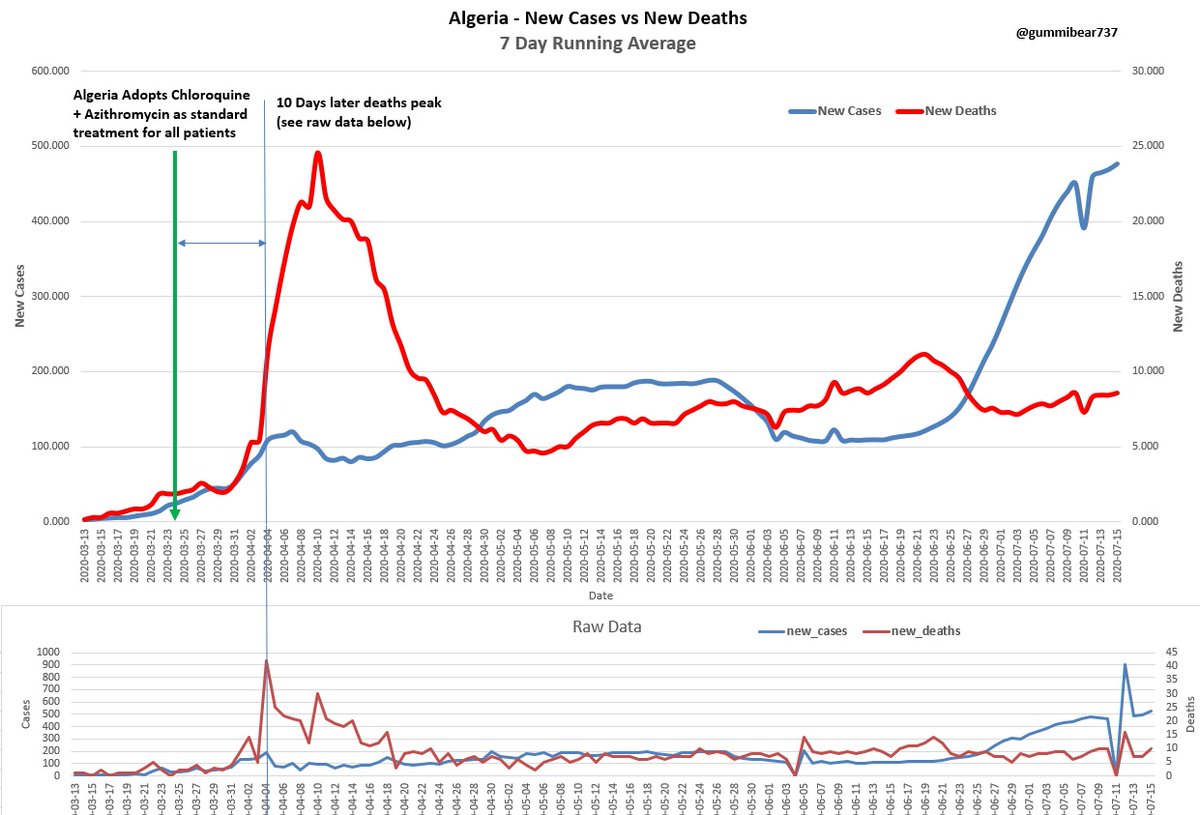
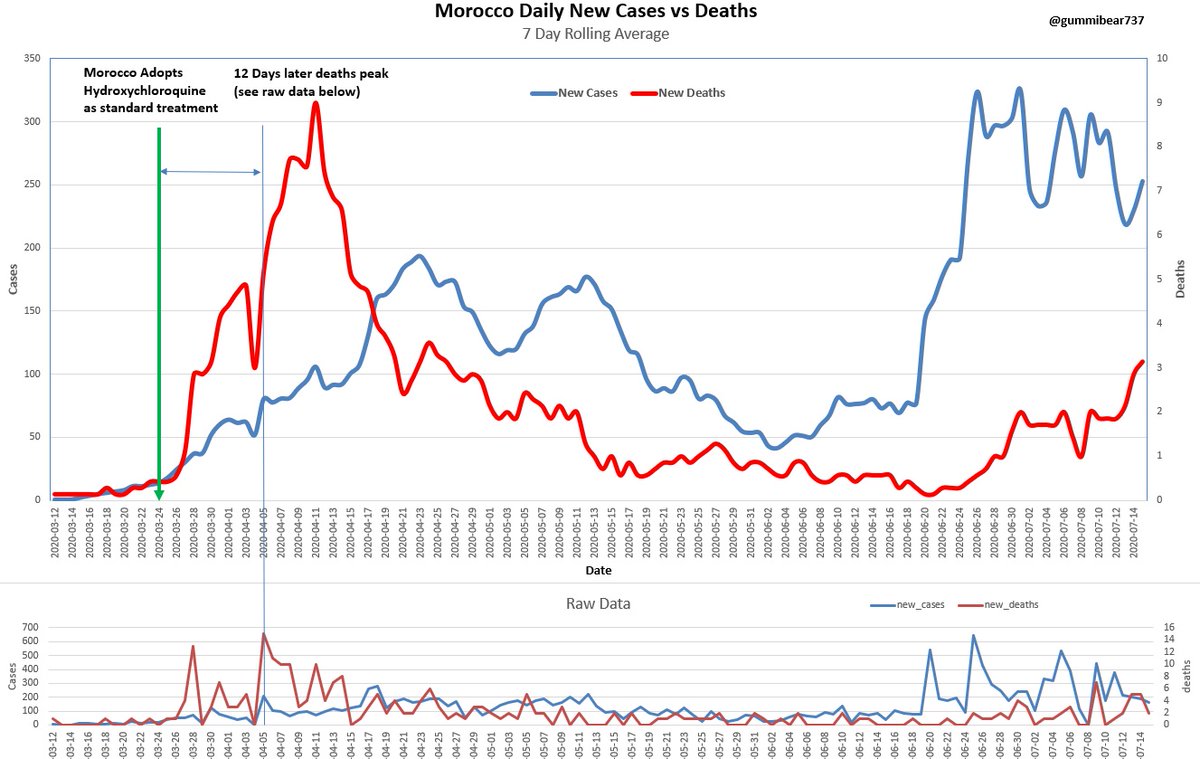






 Palmer Foundation provides an english translation of an interview by Sandro Benites in Portuguese to O Progresso.
Palmer Foundation provides an english translation of an interview by Sandro Benites in Portuguese to O Progresso.