
Love of Theory is the Root of all Evil — Statistician Matthew Briggs
During the pandemic anti-viral treatments were dismissed and their usage cancelled by medical bureaucrats. The rise of “evidence-based medicine” was a major advance in medical science by putting the focus on patient outcomes as the measure of a treatment’s success. Yet during this pandemic in modern western nations, the experiences and observations of primary care physicians and their patients were set aside deliberately in favor of ideology favoring Big Pharma solutions over more available, inexpensive and proven treatment protocols. Pierre Kory suffered directly from this biased, authoritarian discrimination and writes about it in his Real Clear Politics article Censorship Kills: The Shunning of a COVID Therapeutic. Excerpts in italics with my bolds.
Doctors fighting COVID-19 should be supported by their profession and their government, not suppressed. Yet today physicians are smothered under a wave of censorship. With coronavirus variants and vaccine hesitancy threatening a prolonged pandemic, the National Institutes of Health and the broader U.S. medical establishment should free doctors to treat this terrible disease with effective medicines.
For centuries, doctors have addressed emerging health threats by prescribing existing drugs for new uses, observing the results, and communicating to their peers and the public what seems to work. In a pandemic, precious time and lives can be lost by an insistence on excessive data and review. But in the current crisis, many in positions of authority have done just that, stubbornly refusing to allow any repurposed treatments.
This departure from traditional medical practice risks catastrophe. When doctors on the front lines try to bring awareness of and use such medicines, they get silenced.
I’ve experienced such censorship firsthand. Early in the pandemic, my research led me to testify in the Senate that corticosteroids were life-saving against COVID-19, when all national and international health care agencies recommended against them. My recommendations were criticized, ignored and resisted such that I felt forced to resign my faculty position. Only later did a large study from Oxford University find they were indeed life-saving. Overnight, they became the standard of care worldwide. More recently, we identified through dozens of trials that the drug ivermectin leads to large reductions in transmission, mortality, and time to clinical recovery. After testifying to this fact in a second Senate appearance — the video of which was removed by YouTube after garnering over 8 million views — I was forced to leave another position.
I was delighted when our paper on ivermectin passed a rigorous peer review and was accepted by Frontiers in Pharmacology. The abstract was viewed over 102,000 times by people hungry for answers. Six weeks later, the journal suddenly rejected the paper, based on an unnamed “external expert” who stated that “our conclusions were unsupported,” contradicting the four senior, expert peer reviewers who had earlier accepted them. I can’t help but interpret this in context as censorship.
The science shows that ivermectin works. Over 40 randomized trials and observational studies from around the world attest to its efficacy against the novel coronavirus. Meta-analyses by four separate research groups, including ours, found an average reduction in mortality of between 68%-75%. And 10 of 13 randomized controlled trials found statistically significant reductions in time to viral clearance, an effect not associated with any other COVID-19 therapeutic. Furthermore, ivermectin has an unparalleled safety record and low cost, which should negate any fears or resistance to immediate adoption.
Our manuscript conclusions were further supported by the British Ivermectin Recommendation Development (BIRD) Panel. Following the World Health Organization Handbook of Guideline Development, it voted to strongly recommend the use of ivermectin in the treatment and prevention of COVID-19, and opined that further placebo controlled trials are unlikely to be ethical.
Even prior to the BIRD Panel recommendations, many countries have approved the use of ivermectin in COVID-19 or formally incorporated it into national treatment guidelines. Several have gone further and initiated large-scale importation and distribution efforts. In the last month alone, such European Union members as Bulgaria and Slovakia have approved its use nationwide. India, Egypt, Peru, Zimbabwe, and Bolivia are distributing it in many regions and observing rapid decreases in excess deaths. Increasing numbers of regional health authorities have advocated for or adopted it across Japan, Mexico, Brazil, Argentina, and South Africa. And it is now the standard of care in Mexico City, one of the world’s largest cities.
It’s time to stop the foot-dragging. People are dying. The responsible physicians of this country, and their patients, need to be able to rely on their government institutions to quickly identify effective treatments, rather than waiting for pristine, massive Phase III trials before acting. At minimum, the NIH should immediately recommend ivermectin for treating and preventing COVID-19, and then work with professional associations, institutions, and the media to publicize its use.
If it doesn’t, the organization will lose credibility as a public institution charged with acting in the national interest — and doctors will ignore its guidance in the future.
My story is not unique. Physicians across the country are fighting a pernicious campaign to denigrate all potential treatments not first championed by the authorities, and others have faced retaliation for speaking up. Sadly, too many of our institutions are using the pandemic as a pretext to centralize control over the practice of medicine, persecuting and canceling doctors who follow their clinical judgment and expertise.
Actually “following the science” means listening to practitioners and considering the entirety and diversity of clinical studies. That’s exactly what my colleagues and I have done. We won’t be cowed. We will speak up for our patients and do what’s right.
Pierre Kory, MD, is president and chief medical officer of the Front-Line COVID-19 Critical Care Alliance.
Post Script: Evidence from Comparing France and India
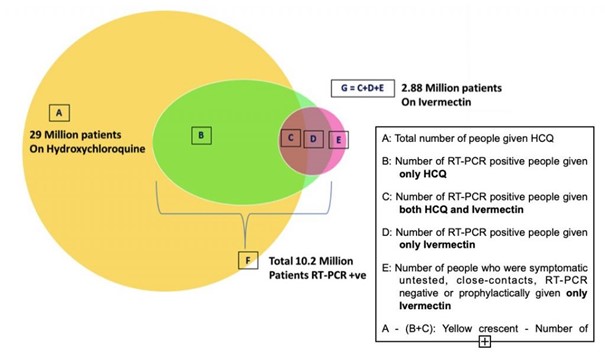
We learn that 30 million Indians have been cured by ivermectin and hydroxychloroquine,
Does there still exist in France a single journalist able to move away from the clandestine restaurant of BFM to look at what is happening outside the ring road?
India has conquered the disease with hydroxychloroquine and ivermectin, uses a traditional vaccine, exports experimental vaccines for these idiotic Westerners
India is the first country in the world for the production of drug molecule, but it is also a developing country. Populated by 1.4 billion inhabitants, it still has 90 million over 60 years also exposed to covid. It is the second country in the world for no number of cases. India followed the Raoult and Borody protocol to the letter …
The rate of reproduction of the virus continues to decline and the country (India) which has known at least 11 million declared cases has reached the threshold of collective immunity.
There are 1,230 deaths per million inhabitants over 65 (six times less than in France). If we had listened to Raoult and followed the Indian model, today we would have 500 cases of covid per day and 75,000 fewer deaths …
Additionally, About those Covid death statistics:
From The Center Square, Illinois: Coroner questions Illinois’ COVID-19 death tally, seeks statewide audit. Excerpts in italics with my bolds.
But a county coroner is calling for a full audit after reviewing some of the deaths in his county.
“My concern is, I’ve reviewed several cases, (of 100 cases) about ten of them here in Monroe County, that the state has deemed COVID-related deaths and none of them have had underlying conditions or contributing factors to COVID,” Monroe County Coroner Bob Hill said. “So my concern is no matter when the person was tested positive, the state is automatically giving them a death classification as related to COVID.”
He said one case in January was an accidental drug overdose, but the decedent had tested positive for COVID-19 in October.
“Don’t automatically put a statistic out there of a (COVID) death when it hasn’t been confirmed what the cause is,” Hill said.
Hill questioned if the motivation to rush reporting of COVID-19 deaths without a full audit was about money.
“The only assumption I can make is the hope the state is seeking some federal money coming down the system for all the numbers of deaths we’ve had due to COVID-19,” Hill said. “That’s the only thing that I can assume. Why else would you want to inflate numbers especially related to COVID.”

Ron,
Have you seen the article “Lockdown – the Big Lie that will never end” at the website Conservative Woman? It may be the best short overview of what is going on with the covid-19 panic that I’ve seen to date.
LikeLike
Thanks rw. See also Tim Black at Spiked on how it went down in UK,
https://www.spiked-online.com/2021/03/26/do-we-now-need-permission-to-be-free/
LikeLike