Covid/Climate Prigs Are Out to Spoil Your Days

Christopher Gage writes at Oxford Sour Bay of Prigs. Excerpts in italics with my bolds.
Enamoured by lockdown, the puritans wish for a perma-pandemic in which no-one, nowhere, will be happy.
Not content with dying their hair green and punching steel through their nostrils, progressives here in Great Britain have proposed something rather more exquisitely demented than their usual fare.
The Independent, a kind of Guardian for actors manqué and Cluster B personalities, those who suffer from fictitious ailments of which ‘the doctor doesn’t know what’s wrong,’ asks, ‘Should Everyone Have a Personal Carbon Quota?’
Helpfully, the newspaper lays out exactly what a Carbon Quota would entail.
It begins: “Your home, sometime in the next decade. You click the heating on and receive an app notification telling you how much of your carbon allowance you’ve used today.
“Outside in the drive, your car’s fuel is linked to the same account. In the fridge, the New Zealand lamb you’ve bought has cost not just pounds and pence but a chunk of this monthly emissions budget too.
“Welcome to the world of personal carbon allowances – a concept that is increasingly gaining traction among experts as a possible response to the climate crisis.”
Curiously, this all sounds like one’s entire life would be recorded and regulated and monitored and meddled with by politicians who’ll punish or praise, all in pursuit of a vague utopia. Sounds familiar.
According to my Carbon Quota, I could live happily and healthily, provided I die next Tuesday at noon.
If I were to stay on this planet and offend Mother Nature with my presence, I’d have to limit myself to half a cigarette per day, a slither of ribeye per week, and one soupçon of red wine per month. Such a paltry regimen would dissolve around 90% of my personality.
Besides, Tuesday is no day to die. Especially before the 4 p.m. happy hour.
Perhaps, I could time it just right. I’ll prop up a stool in my favourite dive bar, and impart everything I’d like to say but avoid saying in fear of social ostracization.
I could say that there is a biological reason why women aren’t funny. I could say that, on balance, the British Empire was a good thing, and that anyone whinging about ‘cultural appropriation’ seldom has any culture worth appropriating. I could say, with conviction, that the Jews obviously don’t secretly run the world because if they did, the world would be far closer to utopia than it is now. I could suggest that those who play music on public transport, indeed—in public—should be hung, drawn, and quartered for the benefit of the gene pool. I could say all this before shuffling off into the light.
(If my girlfriend—whose people have won a fifth of all Nobel Prizes despite being 0.2% of the world population—objects, then I’m sorry… I’m saving the planet, darling.)
You can define the confidence of a culture by the pettiness of its laws.
I’d rather shuffle off than live in a world in which one’s social status is tied to one’s ability to pretend falafel is edible, to one’s withering body. I’d rather that than live in a world in which the prigs and puritans, those weird kids from school with ‘Free Da Weed’ Sharpied on their hemp rucksacks, have won the final victory over everyone else. A world in which every consideration is now suffixed with ‘to save the planet.’
We shouldn’t feign surprise. A stubborn one-third of any population harbours latent authoritarian tendencies. All they need is a little nudge and a wink from someone in a lab coat or a pinstripe suit.
Over the last twenty months, we’ve given them plenty to chew on. We’ve sacralised Crab Mentality—that depressingly human tendency to pull down others into the soup of conformity. For many, this pandemic has been the time of their lives. They’ve enjoyed grassing on neighbours, posting their vaccine statuses, their three-mask chic. Don’t mention that sensible Sweden got it right. Don’t mention that lockdown only delays the inevitable, to great human cost. Don’t mention the fatal link between obesity and Covid deaths.
They’d love life in Austria, where the government has mandated a Western first—forcible vaccination for every citizen.
What a time to be alive. This pandemic has valorised negative personality traits. Back in the Old Normal, high neuroticism combined with high agreeableness meant you’d spend your days siphoning your biography for ‘trauma’ to weaponize against the world. Now, it’s a plus. Like Woke intellectuals, the neurotics mistake their personal problems for societal problems.
I assumed a majority of Britons would, like me, rather chew on a glass vial labelled ‘Wuhan Institute of Virology,’ than consider medical apartheid. Nope.
According to YouGov, six in ten Britons support the introduction of a ‘papers, please’ society—vaccine passports.
That’s despite vaccines blunting Covid’s ability to hospitalise and kill, but not its ability to spread—rendering vaccine passports both pointless and poisonous.
Of course, the usual disclaimer applies just in case anyone of a progressive bent is reading: I’m not saying it’s Nazi Germany, but it’s quite clear how totalitarian regimes slip into power with little resistance.
A recent survey in The Economist made for terrifying reading: forty percent wanted masks forever; a quarter wanted to shut down nightclubs and casinos; another third wanted socially-distanced pubs and clubs and theatres; a hefty rump wanted a 10 p.m. curfew, and one-third said anyone coming into this country should be quarantined, like a dog, for ten days. And they wanted all this lunacy indefinitely, Covid or not.
Perhaps that explains why the eco-loons can air with confidence the drudgery they wish to impose upon everyone else. Not a day goes by without some middle-class Insulate Britain bobo blocking the motorway or making ‘demands’ upon the government to act on the ‘climate crisis’.
What nobody asks is how any of this nonsense would make any difference given that Great Britain contributes less than one percent of global carbon emissions. Those who follow The Science don’t cotton on when last week’s gospel morphs into this week’s heresy.
What happens when we reach Net Zero and the weather doesn’t change? I can only guess… ‘That wasn’t real Net-Zero. Real Net-Zero has never been tried.’
They don’t ask such obvious questions because the answer is obvious: they don’t care about all that. As Mencken wrote, they’re governed by the haunting fear that someone, somewhere, may be happy.
That’s the problem with do-gooding. There’s always more good to do.





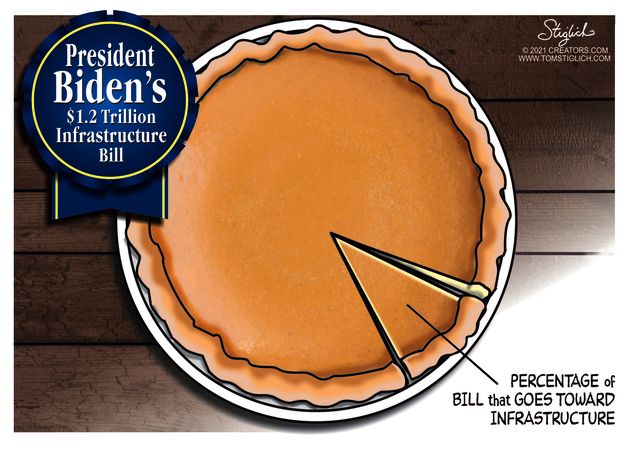 Mathew Kahn discusses the ramifications of the major transportation spending recently passed by the US Congress. Of course, as the pie chart shows, infrastructure as many people think of it—construction or improvement of bridges, highways, roads, rail and subways, ports, waterways, and airports—accounts for only $157 billion, or 7%, of the plan’s estimated cost. Still that is a lot of money (“A billion here, a billion there, and soon it adds up to real money”–US Senator), and Kahn provides a list of concerns in his article
Mathew Kahn discusses the ramifications of the major transportation spending recently passed by the US Congress. Of course, as the pie chart shows, infrastructure as many people think of it—construction or improvement of bridges, highways, roads, rail and subways, ports, waterways, and airports—accounts for only $157 billion, or 7%, of the plan’s estimated cost. Still that is a lot of money (“A billion here, a billion there, and soon it adds up to real money”–US Senator), and Kahn provides a list of concerns in his article