Dr. Richard Urso: End the Pandemic with Early Covid Treatment
Drug Inventor Urso: Are We Underutilizing Early Treatment?
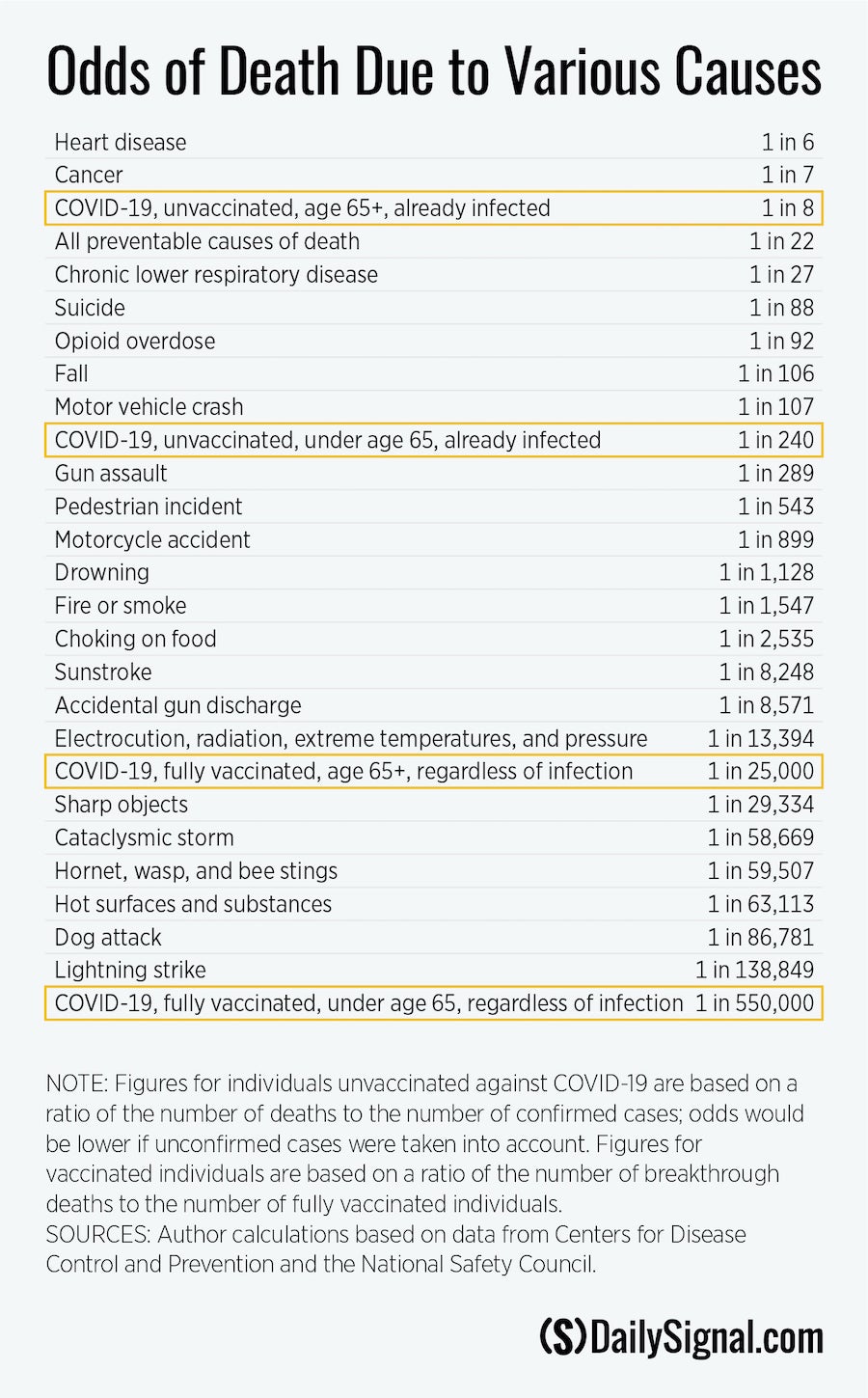
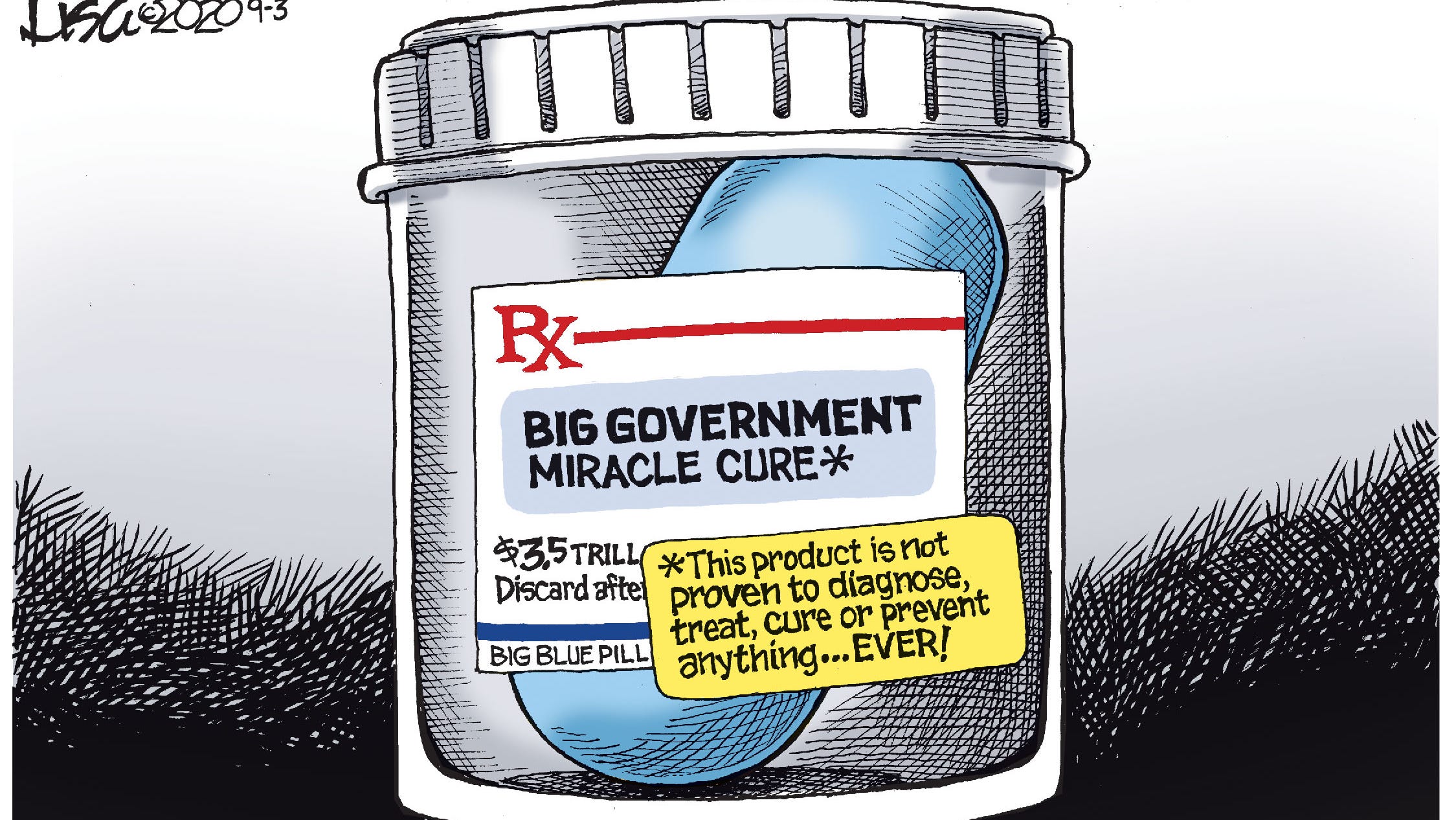
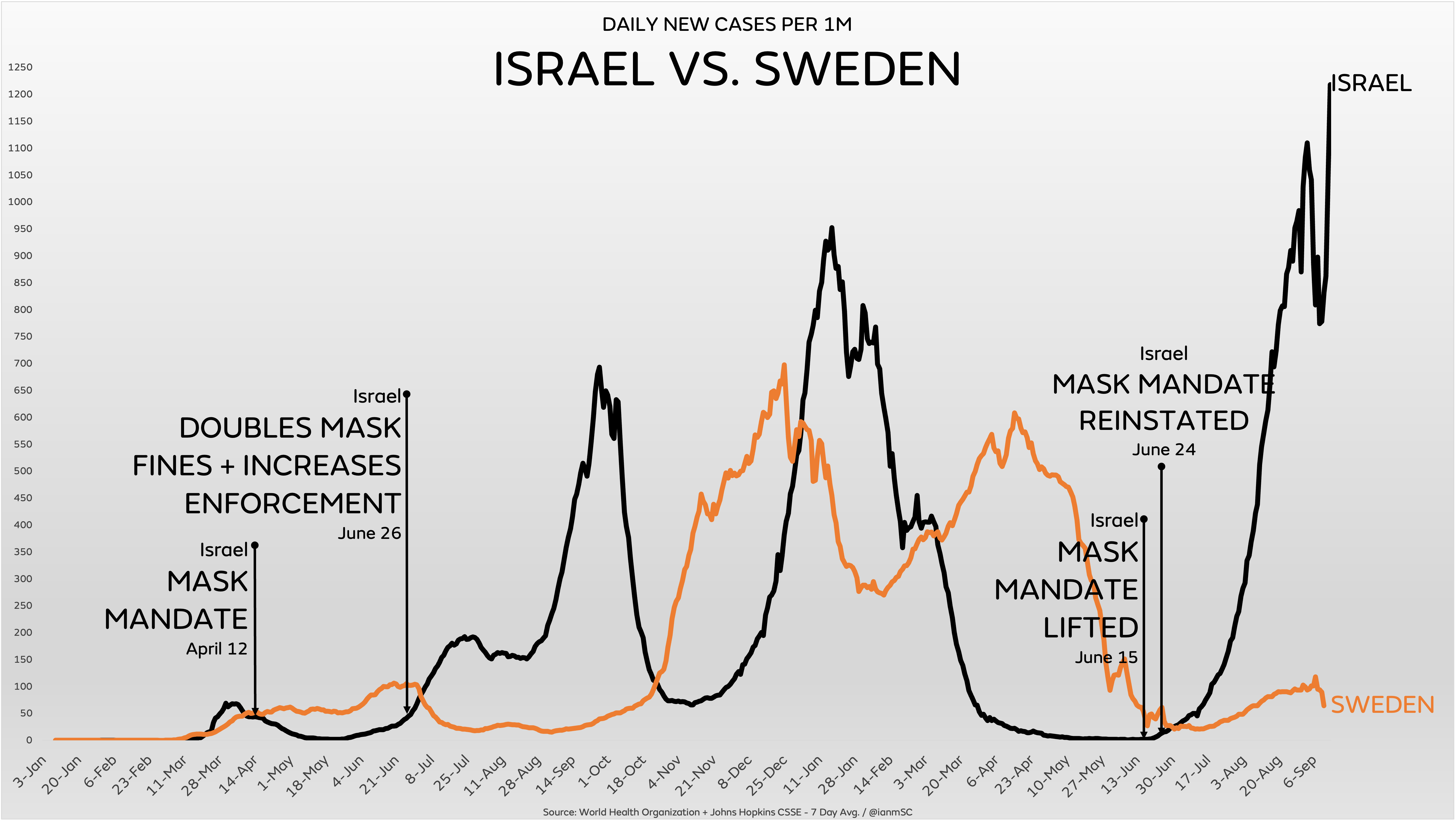
We cannot use a one-size fits all approach to fighting Covid
Dr. Richard Urso is a scientist, sole inventor of an FDA-approved wound healing drug, and the Former Director of Orbital Oncology at MD Anderson Cancer Center. He believes we cannot use a one-size-fits-all approach to fighting Covid.
“We are not going to vaccinate our way out of this,” he said. “There’s no reason to not use anti-inflammatories against inflammatory disease. I used steroids in March and people were saying, ‘Why are you using steroids for inflammatory for this viral disease?’ And I said, ‘Because it’s not a viral disease.’”
Urso says mass lockdowns and waiting for a vaccine never made a lot of sense to him. He calls for a multi-pronged strategy includes targeted vaccination programs, but also early treatment and prevention measures.
“Early treatment should have been part of the equation. I’m not against all those other things. Contagion control is important. Washing our hands. Things like that. They’re all important. Do we need vaccination programs? Absolutely. Do we need early treatment programs? Absolutely. So we have basically put the cart before the horse. The tail is wagging the dog. Early treatment should be a mainstay for everything.”
Background previous post 3000+ Doctors Declaration for Medical Rights and Freedoms

Update October 7: Presently 10,000+ Medical Practitioners have signed this declaration, as well as providing additional resources at Global Covid Summit
By Debra Heine writes at American Greatness Over 3,000 Doctors and Scientists Sign Declaration Accusing COVID Policy-Makers of ‘Crimes Against Humanity’. Excerpts in italics with my bolds and images.
A group of physicians and scientists met in Rome, Italy earlier this month for a three day Global Covid Summit to speak “truth to power about Covid pandemic research and treatment.”
The summit, which was held from September 12 to September 14, gave the medical professionals an opportunity to compare studies, and assess the efficacy of the various treatments that have been developed in hospitals, doctors offices and research labs throughout the world.
The Physicians’ Declaration was first read at the Rome Covid Summit, catalyzing an explosion of active support from medical scientists and physicians around the globe. These professionals were not expecting career threats, character assassination, papers and research censored, social accounts blocked, search results manipulated, clinical trials and patient observations banned, and their professional history and accomplishments altered or omitted in academic and mainstream media.
The document, reprinted below in its entirety, sprang from that conference.
Thousands have died from Covid as a result of being denied life-saving early treatment. The Declaration is a battle cry from physicians who are daily fighting for the right to treat their patients, and the right of patients to receive those treatments – without fear of interference, retribution or censorship by government, pharmacies, pharmaceutical corporations, and big tech. We demand that these groups step aside and honor the sanctity and integrity of the patient-physician relationship, the fundamental maxim “First Do No Harm”, and the freedom of patients and physicians to make informed medical decisions. Lives depend on it.
We the physicians of the world, united and loyal to the Hippocratic Oath, recognizing the profession of medicine as we know it is at a crossroad, are compelled to declare the following;
WHEREAS, it is our utmost responsibility and duty to uphold and restore the dignity, integrity, art and science of medicine;
WHEREAS, there is an unprecedented assault on our ability to care for our patients;
WHEREAS, public policy makers have chosen to force a “one size fits all” treatment strategy, resulting in needless illness and death, rather than upholding fundamental concepts of the individualized, personalized approach to patient care which is proven to be safe and more effective;
WHEREAS, physicians and other health care providers working on the front lines, utilizing their knowledge of epidemiology, pathophysiology and pharmacology, are often first to identify new, potentially life saving treatments;
WHEREAS, physicians are increasingly being discouraged from engaging in open professional discourse and the exchange of ideas about new and emerging diseases, not only endangering the essence of the medical profession, but more importantly, more tragically, the lives of our patients;
WHEREAS, thousands of physicians are being prevented from providing treatment to their patients, as a result of barriers put up by pharmacies, hospitals, and public health agencies, rendering the vast majority of healthcare providers helpless to protect their patients in the face of disease. Physicians are now advising their patients to simply go home (allowing the virus to replicate) and return when their disease worsens, resulting in hundreds of thousands of unnecessary patient deaths, due to failure-to-treat;
WHEREAS, this is not medicine. This is not care. These policies may actually constitute crimes against humanity.
NOW THEREFORE, IT IS:
RESOLVED, that the physician-patient relationship must be restored. The very heart of medicine is this relationship, which allows physicians to best understand their patients and their illnesses, to formulate treatments that give the best chance for success, while the patient is an active participant in their care.
RESOLVED, that the political intrusion into the practice of medicine and the physician/patient relationship must end. Physicians, and all health care providers, must be free to practice the art and science of medicine without fear of retribution, censorship, slander, or disciplinary action, including possible loss of licensure and hospital privileges, loss of insurance contracts and interference from government entities and organizations – which further prevent us from caring for patients in need. More than ever, the right and ability to exchange objective scientific findings, which further our understanding of disease, must be protected.
RESOLVED, that physicians must defend their right to prescribe treatment, observing the tenet FIRST, DO NO HARM. Physicians shall not be restricted from prescribing safe and effective treatments. These restrictions continue to cause unnecessary sickness and death. The rights of patients, after being fully informed about the risks and benefits of each option, must be restored to receive those treatments.
RESOLVED, that we invite physicians of the world and all health care providers to join us in this noble cause as we endeavor to restore trust, integrity and professionalism to the practice of medicine.
RESOLVED, that we invite the scientists of the world, who are skilled in biomedical research and uphold the highest ethical and moral standards, to insist on their ability to conduct and publish objective, empirical research without fear of reprisal upon their careers, reputations and livelihoods.
RESOLVED, that we invite patients, who believe in the importance of the physician-patient relationship and the ability to be active participants in their care, to demand access to science-based medical care.








 John P.A. Ioannidis writes at The Tablet
John P.A. Ioannidis writes at The Tablet