As the world wearies of trying to suppress the SARS-CoV-2 virus, many of us are wondering what the future will look like as we try to learn to live with it.
Will it always have the capacity to make us so sick? Will our immune systems learn — and remember — how to cope with the new threat? Will vaccines be protective and long-lasting?
STAT asked a number of experts to map out scenarios of how we might come to coexist with this new threat. In a time of uncertainty, the scenarios they sketched were actually hopeful, even if the relief most envisage is not immediately around the corner.
Vineet Menachery, a coronavirus researcher at the University of Texas Medical Branch in Galveston laid out four possible scenarios for how humans might interact with SARS-2 over time — in other words, what kind of immunity we might expect.
As Menachery sees it, the possibilities for the future when it comes to Covid-19 and human immunity break down as follows:
sterilizing immunity,
functional immunity,
waning immunity, and
lost immunity.
Please remember: These are educated guesses, based on what’s known about the way the immune system works in general, and how it responds to other coronaviruses.
Sterilizing immunity
Sterilizing immunity would be a best-case scenario. It describes an immune system that is armed against a foe, able to fend it off before infection can take hold.
Diseases that we think of as “one-and-done” infections induce such a robust and durable immune response in a single encounter that we cannot be reinfected. In general terms, measles fits into this category, although there are rare reports of people contracting measles more than once.
The bad news is that viruses that infect via the mucus membranes of the nose and throat, like SARS-2, typically don’t induce sterilizing immunity.
But Florian Krammer, a professor of vaccinology at the Icahn School of Medicine at Mount Sinai Hospital in New York, does believe some people will develop sterilizing immunity after a bout of Covid-19.
Malik Peiris, a coronavirus expert at the Hong Kong University who was one of the co-discoverers of SARS-1, said, “Of course, what we’d all like is immunity that protects the individual — protects from infection and protects from transmission. We may not achieve that, because protecting from infection of the upper respiratory tract and then transmission is quite a challenge.”
Functional immunity
Functional immunity, on the other hand, may be within reach. In fact, it’s the scenario Menachery sees as most likely.
Under this scenario, people whose immune systems have been primed to recognize and fight the virus — whether through infection or vaccination — could contract it again in the future. But these infections would be cut short as the immune system’s defenses kick into gear. People infected might not develop symptoms or might have a mild, cold-like infection.
“I’m a believer that if you’ve gotten Covid-19, then your likelihood of dying from a second Covid-19 case is very low, if you maintain immunity,” Menachery said.
Peiris agreed. “It won’t have the impact it has now. … It becomes manageable.” “The fact that somebody may get reinfected is not surprising. But the reinfection didn’t cause disease,” said Peiris, who knows about the case but was not one of the authors reporting it.
Christian Drosten, who is another co-discoverer of SARS-1, describes a future that fits into this category.
“I clearly expect lasting and relevant immunity that is almost sterilizing immunity against SARS-2 in almost every person infected with SARS-2,” Drosten, director of the Institute of Virology at Berlin’s Charité University Hospital, said via email.
“It may be possible to become infected again, without any change in the virus. The resulting infection will be mild or asymptomatic, with significantly lower levels of virus replication and onward transmission.”
Drosten’s last point would be a big bonus. If people who are reinfected don’t generate high levels of SARS-2 viruses in their respiratory tracts and therefore don’t contribute much to the spread of the virus, Covid-19 may become, over time, not just less dangerous, but also less common.
Waning immunity
Waning infection, the third scenario, is a variation of functional immunity. In this scenario, people who have been infected or vaccinated would lose their protection over time. But even if immunity wanes, reinfections would be less severe, Menachery said.
“You will never get as sick as you were the first time,” he said.
This is the pattern seen with the four coronaviruses that cause about 15% of what we consider common colds — OC43, 229E, NL63, and HKU1. People can be reinfected with these viruses after a relatively short period of time.
Thirty years ago, British scientists reported that a year after deliberately infecting a small number of volunteers with 229E, two-thirds became reinfected when again exposed to the virus. “However, the period of virus shedding was shorter than before and none developed a cold,” they wrote.
Krammer believes the overall picture will be mixed. Some people will have sterilizing immunity, but most will fit into either the functional or waning immunity categories. The net outcome: less of the type of disease that prompted most countries to take the extraordinary steps of locking down this spring.
Lost immunity
Lost immunity describes a scenario in which people who have been infected would lose all their immune munitions against the virus within some time frame. A reinfection after that point would be like a first infection — carrying all the same risk of severe disease now seen with Covid-19.
None of the experts who spoke to STAT felt this was a possibility.
“I can’t imagine this being a situation where I get infected and then in 10 years, I get infected again and I have zero immunity,” Perlman said.
If these experts are correct, and the worst-case scenario is off the table, humans can expect to see a waning of the threat SARS-2 poses to people over time. Our immune systems will know how to deal with it. It could become the fifth human coronavirus to cause common colds.
But leaving all that aside, and leaving aside my personal feeling that masks are more of a placebo than anything, I am willing to lean on my previously stated understanding of national compromise and don the mask. I’m even willing to admit that I might be wrong about my feelings on masks. I will concede all of that. The problem is that the other side of this debate isn’t willing to concede a single inch. All or nothing is a dangerous game, especially when it is only one side that agrees to it. Reasonable people who are forced into unreasonable acts can only be stretched so far. When they snap they will retreat to “nothing” and then that’s when real problems start. We can already see that happening.
As Edit0r-at-Large for a major online publication, I am not only tasked with staying abreast of the statistics and data connected to COVID, my writers are having daily, extended conversations about the information regarding the virus, transmission and fatality rates and recovery rates. In fact, we report factual statistics most corporate media sites have never published at all. There is a constant distillation of the issue going on behind the scenes here every single day.
I say this to explain that while I’m no Expert Scientist™, I am informed. I also believe that my willingness to compromise demonstrates an ability to reason effectively. So it has become infuriating, to the point of feeling untenable, that the “lockdown indefinitely” crowd has become so unhinged as to label people like me morons, “deniers” and pro-murder because we find the reaction to this virus outsized and dangerous.
But Kira, you can’t compromise on DEATH! Why do you hate the elderly????
Can’t we? We compromise on death every day, pandemic or not. We calculate the risk to drive our vehicles, attend events, get on airplanes. We use a complicated equation based on what facts we know, our fears and our goals. If this virus had the fatality rate we were promised in the beginning, extended lockdowns might…might…be defensible. But we are looking at a virus with a 99.6% survivability rate. For the elderly that rate is certainly different. The solution is not to quarantine the healthy. We’ve never done that. Ever.
The solution is to quarantine the sick, encourage healthy habits and safe interactions among the healthy, and GET THE HELL ON WITH LIVING WHILE WE’RE STILL ALIVE.
We are shutting down schools when the total number of child fatalities in the entire nation stands somewhere between ten and two, depending on how you count COVID deaths. Even the Mayo Clinic says nearly all children who get the virus will never even show symptoms or only experience mild symptoms.
But Kira, the teachers and the staff are more vulnerable. Why do you hate teachers???
There are many teachers and staff who feel just fine about returning to the classroom. In K-12 education, teachers tend to skew younger and have a much lower risk. Of course, that shifts quite a bit when it comes to college professors. Invite those who feel comfortable to return to campus with the students. Those who don’t feel comfortable should Zoom in to the classroom, ideally one supervised by aides and subs. The unions are always begging for more hires. This seems like a no-brainer.
But Kira, nearly 200,000 people are dead because of COVID. Why do you hate people???
I have made my case for my informed status on this issue. I know the numbers. We are far, far, far, far, far, far shy of the 3-5 million deaths Fauci and co. promised in the beginning of all this. Even with quarantine measures we were told millions would still die. In a population of 325 million, 174,000 is statistically negligible.
But Kira, you heartless monster! How can you say you don’t care about all those people who died?
And herein lies the rub, the very heart of this rant today. I have no belief whatsoever that those screaming at me about how little I care for the lives of others actually care for the lives of those others themselves. My opinion that a virus with a 99.6% survivability rate should not bring a successful society to a screeching halt does not denote my malice for my fellow Americans. Quite the opposite.
I care very much about the daily suffering I see as people lose their jobs, businesses, and even their mental stability to this ridiculous response.
I have been patient. I have been a good citizen. I have done everything asked of me. I have tried to be gracious to those who insult my intelligence and qualifications simply because I don’t see things their way. I have tried to understand that people are scared and that not everyone has all the information and I can’t force them to have it. I have chosen the path of acceptance for those who rage and seethe and hiss all day on social media about people like me, people who have the audacity to even suggest perhaps it’s time for citizens to be making these decisions for themselves. I have genuinely tried to be the bigger person. I don’t post memes insulting people who want to wear masks, even as many of my friends and family regularly and smugly post memes insulting those of us who have questions about it all.
But I’ve had enough. The fact that we even have the space or notion to argue about the responses to this virus tells me that indeed this virus is not the apocalypse we were told it would be. I will not be judged or labeled as heartless for a simple reading of the facts available to me. I will not be told I don’t care about people when all I do all day long is worry for people and pray for people and entreat God to protect our people. I will not be shamed as a murderer for thinking maybe it’s time to start living again.
Over the first three years of his Administration, President Donald J. Trump used a combination of tax cuts, deregulation, energy dominance, and fair trade deals to build one of the most robust and resilient economies in American history. As a result of these growth-inducing policies,by January 20, 2020 – the day the Chinese Communist Party confirmed human-to-human transmission of SARS-CoV-2 – the United States economy was at full employment,1 real wages were rising,2 and black and Hispanic Americans were enjoying record low unemployment rates. 3.
Since that time, SARS-CoV-2 – hereinafter referred to as the China Virus – has taken a horrific toll. Over 160,000 Americans have died.4 As many as 18 million Americans are currently unemployed.5 Trillions of dollars of fiscal and monetary stimuli have been expended to combat the sharpest and deepest economic downturn in U.S. history. 6
Today, the U.S. economy is also in the midst of profound structural changes in sectors heavily impacted by the China Virus such as airlines and mass transit, casinos and gaming, K-12 and higher education, hospitality and leisure, oil and gas drilling, and sports and entertainment. These structural impacts could have long-lasting consequences.
Just how did this happen? And how is President Trump using the Defense Production Act (DPA) and related tools such as the 2020 Coronavirus Aid, Relief, and Economic Security (CARES) Act to protect the American people from the China Virus? This report seeks to answer these questions.
Table of Contents
The Chinese Communist Party Causes a Global Pandemic
Overview of the Defense Production Act.
The Strategic National Stockpile and DPA Mission
Executive Orders and Presidential Memoranda
Using DPA Title I to Attack the China Virus
Using DPA Title III to Attack the China Virus
CARES Act and PPP Funding to Supplement DPA Efforts
Patriotic Companies Answering the Call to Duty
Conclusion
The China Virus outbreak is an invisible enemy unlike any in modern history. The intentional shielding of the outbreak by the Chinese Communist Party and World Health Organization virtually ensured the outbreak of a global pandemic that has killed over 160,000 Americans and inflicted great damage on the American economy.
Using the DPA and other authorities, President Trump has moved quickly to protect the American people and defend our industrial base. His aggressive use of the DPA has not only saved American lives during this pandemic. It is helping to protect and secure America’s production and distribution of our essential medicines and critical medical equipment and supplies.
On Aug. 10 the FDA denied the urgent request for emergency approval for COVID-19 outpatient preventive and early treatment use of hydroxychloroquine (HCQ) filed July 1 by Dr. John McKinnon’s team at Henry Ford Hospital in Detroit, supported by Dr. Peter McCullough’s cardiology team at Baylor Heart and Vascular Institute in Dallas.
Approximately 48,000 more Americans have died during the FDA’s 48-day delay since this Emergency Use Authorization (EUA) was requested on July 1. Dr. McKinnon’s clinical trial found an impressive 51% reduction in deaths if HCQ was begun within 24 hours of admission to the hospital.
An outpatient primary care study by Dr. Vladimir Zelenko, using HCQ, azithromycin and zinc given within less than seven days of COVID-19 symptoms, showed approximately 80% decrease in deaths, and less than 1% of his patients needed to be hospitalized. These extraordinary results show how many lives can be saved with early HCQ treatment.
Dr. Harvey Risch, Yale epidemiologist, projected that widespread early treatment for COVID-19 with HCQ could have saved 100,000 American lives.
The physician head of the FDA, Dr. Steven Hahn, has again betrayed physicians and patients by preventing Americans from having the “right to try” HCQ for early COVID-19 treatment. Dr. Hahn knows full well the FDA approved HCQ as safe in 1955, and it has been used in millions of patients worldwide for 65 years with an impressive track record of safety in patients of all ages, all ethnic groups, and even pregnant women and nursing mothers.
The FDA’s denial of the EUA for early outpatient COVID-19 use of HCQ continues the agency’s false narrative in claiming outpatient harm for HCQ, based on inpatient data in critically ill patients. Dr. Hahn has ignored established facts of effectiveness and lack of harm for outpatients that have been established in more than 50 recent studies.
A newly released study from Turkeyfound no cardiac abnormalities with HCQ given at therapeutic doses for five days in early COVID patients. Attributing any late-stage cardiac effects to HCQ that is known to be caused by the virus and inflammatory damage is indefensible.
What amount of “data” will ever satisfy Dr. Hahn?
The FDA used a standard of “may be effective” for the rapid May 1 EUA given to the experimental anti-viral remdesivir, based on one controlled clinical trial terminated early. Yet FDA is now requiring a higher standard of a randomized controlled clinical trial for the already FDA-approved HCQ in safe use for 65 years. Remdesivir showed very little benefit shown in hospitalized COVID patients and had serious side effects.
Nine of the members of the NIH panel relied on for COVID treatment advice were supported financially by Gilead Sciences, maker of remdesivir.
As a cancer specialist, Dr. Hahn knows early treatment of any disease is critical, especially viral illness. But it is more critical with COVID-19, or SARS CoV-2, as we learned in 2005 when National Institutes of Health (NIH) and Centers for Disease Control and Prevention (CDC) published their studies from the 2002 outbreak of the closely related SARS-CoV-1 virus. These laboratory tests of possible anti-viral medicines clearly showed potent antiviral effects of chloroquine (CQ) against SARS-CoV-1 to block the SARS-CoV-1 infection at the earliest stage. Dr. Fauci was at NIH them, so he has known about this work for more than 15 years.
From these studies we know that HCQ with zinc works during the first five days to stop viral entry into our cells and to block the virus from multiplying.
Without HCQ and zinc, by day six or seven the viral load explodes and then triggers an exaggerated inflammatory response. This “cytokine storm” can severely damage critical organs: lungs, kidneys, heart, brain, liver and intestines and is often fatal.
Earlier this year, Dr. Peter McCullough’s team showed prophylactic benefits of HCQ given to hospital workers who were exposed to COVID daily in their work, just as found in India, South Korea, China and multiple other countries.
This preventive benefit of HCQ given once a week could protect front-line medical workers, law enforcement officers, paramedics, clergy, dentists/dental hygienists, truck drivers, food-processing workers, teachers, behavioral health professionals, factory and grocery store workers, flight attendants and many others. We could more safely reopen America’s businesses, schools and churches with doctors and patients having widespread, early access to HCQ.
Doctors treating COVID-19 patients NOW see lives being saved by cheap, safe, FDA-approved medicines – hydroxychloroquine with azithromycin or doxycycline, plus supplemental zinc, vitamin C and vitamin D.
Why don’t Americans have the freedom to use HCQ here as in other countries?
The FDA’s misleading statements about HCQ have led to dangerous, unprecedented restrictions on physicians’ off-label prescribing rights imposed by state governors, medical boards and pharmacy boards. The supply of HCQ has been ramped up to handle its use in early treatment of COVID. The Strategic National Stockpile has millions of doses deteriorating in government warehouses that are not being distributed because doctors are prevented for political reasons from prescribing for outpatients with COVID-19.
Americans are dying needlessly for political and financial agendas waiting for the “magic bullet” of a vaccine, not due to lack of available treatment for COVID-19. We still need therapeutics, such as HCQ, even if a vaccine works and is safe.
Testing is inaccurate and often unavailable, and HCQ dispensing must not be limited to persons with a positive test. Such limits also prevent prophylactic use. Governors and bureaucrats must not be allowed to arbitrarily restrict life-saving HCQ treatment.
The Fauci-Hahn strategies of suppressing the positive studies of HCQ effectiveness for outpatient use, while focusing on mandatory mask edicts and continued shutdowns of businesses, schools and churches are not controlling the pandemic. These political agendas have eroded our constitutional freedoms and devastated our financial, psychological, physical and spiritual well-being – while costing 1,000 American lives every day.
Dr. Hahn needs to be held accountable for the preventable deaths caused on his watch. As a physician licensed in three states that prevent prescribing HCQ for my patients, I submitted a formal request to the chairman of Senate Oversight Committee on Homeland Security and Governmental Affairs (HSGAC) for Dr. Hahn to be called before the Committee to produce the data on which the FDA is claiming “harm” in using HCQ for outpatients in the mild stage of COVID, but no such harm for RA, Lupus, or malaria. FDA’s hypocrisy ignores their own safety data, basic science, clinical studies and common sense.
Americans must speak out and demand the medical freedom to consult their physicians and decide treatment options without government interference.
We live in a culture that has uncritically accepted that every domain of life is political, and that even things we think are not political are so, that all human enterprises are merely power struggles, that even the idea of “truth” is a fantasy, and really a matter of imposing one’s view on others. For a while, some held out hope that science remained an exception to this. That scientists would not bring their personal political biases into their science, and they would not be mobbed if what they said was unwelcome to one faction or another. But the sordid 2020 drama of hydroxychloroquine—which saw scientists routinely attacked for critically evaluating evidence and coming to politically inconvenient conclusions—has, for many, killed those hopes.
Phase 1 of the pandemic saw the near collapse of the credible authority of much of our public health officialdom at the highest levels, led by the exposure of the corruption of the World Health Organization. The crisis was deepened by the numerous reversals on recommendations, which led to the growing belief that too many officials were interpreting, bending, or speaking about the science relevant to the pandemic in a politicized way. Phase 2 is equally dangerous, for it shows that politicization has started to penetrate the peer review process, and how studies are reported in scientific journals, and of course in the press.
What is unique about the hydroxychloroquine discussion is that it is a story of “unwishful thinking”—to coin a term for the perverse hope that some good outcome that most sane people would earnestly desire, will never come to pass. It’s about how, in the midst of a pandemic, thousands started earnestly hoping—before the science was really in—that a drug, one that might save lives at a comparatively low cost, would not actually do so. Reasonably good studies were depicted as sloppy work, fatally flawed. Many have excelled in making counterfeit bills that look real, but few have excelled at making real bills look counterfeit. As such, as we sort this out, we shall observe not only some “tricks” about how to make bad studies look like good ones, but also how to make good studies look like bad ones. And why should anyone facing a pandemic wish to discredit potentially lifesaving medications? Well, in fact, this ability can come in very handy in this midst of a plague, when many medications and vaccines are competing to Save the World—and for the billions of dollars that will go along with that.
So this story is twofold. It’s about the discussion that unfolded (and is still unfolding) around hydroxychloroquine, but if you’re here for a definitive answer to a narrow question about one specific drug (“does hydroxychloroquine work?”), you will be disappointed. Because what our tale is really concerned with is the perilous state of vulnerability of our scientific discourse, models, and institutions—which is arguably a much bigger, and more urgent problem, since there are other drugs that must be tested for safety and effectiveness (most complex illnesses like COVID-19 often require a group of medications) as well as vaccines, which would be slated to be given to billions of people. “This misbegotten episode regarding hydroxychloroquine will be studied by sociologists of medicine as a classic example of how extra-scientific factors overrode clear-cut medical evidence,” Yale professor of epidemiology Harvey A. Risch recently argued. Why not start studying it now?
Norman Doige tells the story in some detail (see article link in red at the top)
the history of quinine, chloroquine, and HCQ medical effectiveness;
how HCQ was used against SARS CV2 early on;
how Raoult was the one in his lab who came up with the idea of combining the two older drugs, HCQ and azithromycin, for COVID-19;
the criticisms of the French studies exemplifying “unwishful thinking”;
Trump’s interest in HCQ and the media backlash against the medicine;
the failure of ICU treatment protocols with ventilators and no alternatives to off-label prescribing;
the insistence upon Randomized Controlled Trials (RCTs) as the only valid test for HCQ;
the confounding factors in such studies and the problems replicating RCT results; and,
the publication in high-profile journals of studies structured for HCQ to fail to help infected patients.
Conclusion from Doige
Lots and lots of COVID-19 studies will come out—several hundred are in the works. People will hope more and more accumulating numbers—and more big data—will settle it. But big data, interpreted by people who have never treated any of the patients involved can be dangerous, a kind of exalted nonsense. It’s an old lesson: Quantity is not quality.
On this, I favor the all-available-evidence approach, which understands that large studies are important, but also that the medication that might be best for the largest number of people may not be best one for an individual patient. In fact, it would be typical of medicine that a number of different medications will be needed for COVID-19, and that there will be interactions of some with patient’s existing medications or conditions, so that the more medications we have to choose from, the better. We should be giving individual clinicians on the front lines the usual latitude to take account of their individual patient’s condition, and preferences, and encourage these physicians to bring to bear everything they have learned and read (they have been trained to read studies), and continue to read, but also what they have seen with their own eyes. Unlike medical bureaucrats or others who issue decrees from remote places physicians are literally on our front lines—actually observing the patients in question, and a Hippocratic Oath to serve them—and not the Lancet or WHO or CNN.
As contentious as this debate has been, and as urgent as the need for informed and timely information seems now, the reason to understand what happened with HCQ is for what it reflects about the social context within which science is now produced:
a landscape overly influenced by technology and its obsession with big data abstraction over concrete, tangible human experience;
academics who increasingly see all human activities as “political” power games, and so in good conscience can now justify inserting their own politics into academic pursuits and reporting;
extraordinarily powerful pharmaceutical companies competing for hundreds of billions of dollars;
politicians competing for pharmaceutical dollars as well as public adoration—both of which come these days too much from social media; and,
the decaying of the journalistic and scholarly super-layers that used to do much better holding everyone in this pyramid accountable, but no longer do, or even can.
If you think this year’s controversy is bad, consider that hydroxychloroquine is given to relatively few people with COVID-19, all sick, many with nothing to lose. It enters the body, and leaves fairly quickly, and has been known to us for decades. COVID vaccines, which advocates will want to be mandatory and given to all people—healthy and not, young and old—are being rushed past their normal safety precautions and regulations, and the typical five-to-10-year observation period is being waived to get “Operation Warp Speed” done as soon as possible.
This is being done with the endorsement of public health officials—the same ones, in many cases who are saying HCQ is suddenly extremely dangerous.
Philosophically, and psychologically, it is a fantastic spectacle to behold, a reversal, the magnitude and the chutzpah of which must inspire awe: a public health establishment, showing extraordinary risk aversion to medications and treatments that are extremely well known, and had been used by billions, suddenly throwing caution to the wind and endorsing the rollout of treatments that are entirely novel—and about which we literally can’t possibly know anything, as regards to their long-term effects. Their manufacturers know this well themselves, which is why they have aimed for, insisted on, and have already been granted indemnification—guaranteed, by those same public health officials and government that they will not be held legally accountable should their product cause injury.
From unheard of extremes of caution and “unwishful thinking,” to unheard of extremes of risk-taking, and recklessly wishful thinking, this double standard, this about-face, is not happening because this issue of public safety is really so complex a problem that only our experts can understand it; it is happening because there is, right now, a much bigger problem: with our experts, and with the institutions that we had trusted to help solve our most pressing scientific and medical problems.
Unless these are attended to, HCQ won’t be remembered simply as that major medical issue that no one could agree on, and which left overwhelming controversy, confusion, and possibly unnecessary deaths of tens of thousands in its wake; it will be one of many in a chain of such disasters.
Norman Doidge, a contributing writer for Tablet, is a psychiatrist, psychoanalyst, and author of The Brain That Changes Itself and The Brain’s Way of Healing.
The map shows that in Canada 9206 deaths have been attributed to Covid19, meaning people who died having tested positive for SARS CV2 virus. This number accumulated over a period of 198 days starting January 31. The daily death rate reached a peak of 177 on May 6, 2020, and is down to 6 as of yesterday. More details on this below, but first the summary picture. (Note: 2019 is the latest demographic report)
Canada Pop
Ann Deaths
Daily Deaths
Risk per Person
2019
37589262
330786
906
0.8800%
Covid 2020
37589262
9206
46
0.0245%
Over the epidemic months, the average Covid daily death rate amounted to 5% of the All Causes death rate. During this time a Canadian had an average risk of 1 in 5000 of dying with SARS CV2 versus a 1 in 114 chance of dying regardless of that infection. As shown later below the risk varied greatly with age, much lower for younger, healthier people.
Background Updated from Previous Post
In reporting on Covid19 pandemic, governments have provided information intended to frighten the public into compliance with orders constraining freedom of movement and activity. For example, the above map of the Canadian experience is all cumulative, and the curve will continue upward as long as cases can be found and deaths attributed. As shown below, we can work around this myopia by calculating the daily differentials, and then averaging newly reported cases and deaths by seven days to smooth out lumps in the data processing by institutions.
A second major deficiency is lack of reporting of recoveries, including people infected and not requiring hospitalization or, in many cases, without professional diagnosis or treatment. The only recoveries presently to be found are limited statistics on patients released from hospital. The only way to get at the scale of recoveries is to subtract deaths from cases, considering survivors to be in recovery or cured. Comparing such numbers involves the delay between infection, symptoms and death. Herein lies another issue of terminology: a positive test for the SARS CV2 virus is reported as a case of the disease COVID19. In fact, an unknown number of people have been infected without symptoms, and many with very mild discomfort.
August 7 in the UK it was reported (here) that around 10% of coronavirus deaths recorded in England – almost 4,200 – could be wiped from official records due to an error in counting. Last month, Health Secretary Matt Hancock ordered a review into the way the daily death count was calculated in England citing a possible ‘statistical flaw’. Academics found that Public Health England’s statistics included everyone who had died after testing positive – even if the death occurred naturally or in a freak accident, and after the person had recovered from the virus. Numbers will now be reconfigured, counting deaths if a person died within 28 days of testing positive much like Scotland and Northern Ireland…
Professor Heneghan, director of the Centre for Evidence-Based Medicine at Oxford University, who first noticed the error, told the Sun:
‘It is a sensible decision. There is no point attributing deaths to Covid-19 28 days after infection…
For this discussion let’s assume that anyone reported as dying from COVD19 tested positive for the virus at some point prior. From the reasoning above let us assume that 28 days after testing positive for the virus, survivors can be considered recoveries.
Recoveries are calculated as cases minus deaths with a lag of 28 days. Daily cases and deaths are averages of the seven days ending on the stated date. Recoveries are # of cases from 28 days earlier minus # of daily deaths on the stated date. Since both testing and reports of Covid deaths were sketchy in the beginning, this graph begins with daily deaths as of April 24, 2020 compared to cases reported on March 27, 2020.
The line shows the Positivity metric for Canada starting at nearly 8% for new cases April 24, 2020. That is, for the 7 day period ending April 24, there were a daily average of 21,772 tests and 1715 new cases reported. Since then the rate of new cases has dropped down, now holding steady at ~1% since mid-June. Yesterday, the daily average number of tests was 47,221 with 377 new cases. So despite more than doubling the testing, the positivity rate is not climbing. Another view of the data is shown below.
The scale of testing has increased and has now reached nearly 50,000 a day, while positive tests (cases) are hovering at 1% positivity. The shape of the recovery curve resembles the case curve lagged by 28 days, since death rates are a small portion of cases. The recovery rate has grown from 83% to 98% steady over the last 3 weeks, so that recoveries now exceed new positives. This approximation surely understates the number of those infected with SAR CV2 who are healthy afterwards, since antibody studies show infection rates multiples higher than confirmed positive tests (8 times higher in Canada). In absolute terms, cases are now down to 377 a day and deaths 6 a day, while estimates of recoveries are 386 a day.
Summary of Canada Covid Epidemic
It took a lot of work, but I was able to produce something akin to the Dutch advice to their citizens.
The media and governmental reports focus on total accumulated numbers which are big enough to scare people to do as they are told. In the absence of contextual comparisons, citizens have difficulty answering the main (perhaps only) question on their minds: What are my chances of catching Covid19 and dying from it?
A previous post reported that the Netherlands parliament was provided with the type of guidance everyone wants to see.
The table presents only those cases with a full clinical documentation, which included some 2194 deaths compared to the 5842 total reported. The numbers show that under 60 years old, few adults and almost no children have anything to fear.
Update May 20, 2020
It is really quite difficult to find cases and deaths broken down by age groups. For Canadian national statistics, I resorted to a report from Ontario to get the age distributions, since that province provides 69% of the cases outside of Quebec and 87% of the deaths. Applying those proportions across Canada results in this table. For Canada as a whole nation:
Age
Risk of Test +
Risk of Death
Population per 1 CV death
<20
0.05%
None
NA
20-39
0.20%
0.000%
431817
40-59
0.25%
0.002%
42273
60-79
0.20%
0.020%
4984
80+
0.76%
0.251%
398
In the worst case, if you are a Canadian aged more than 80 years, you have a 1 in 400 chance of dying from Covid19. If you are 60 to 80 years old, your odds are 1 in 5000. Younger than that, it’s only slightly higher than winning (or in this case, losing the lottery).
As noted above Quebec provides the bulk of cases and deaths in Canada, and also reports age distribution more precisely, The numbers in the table below show risks for Quebecers.
Age
Risk of Test +
Risk of Death
Population per 1 CV death
0-9 yrs
0.13%
0
NA
10-19 yrs
0.21%
0
NA
20-29 yrs
0.50%
0.000%
289,647
30-39
0.51%
0.001%
152,009
40-49 years
0.63%
0.001%
73,342
50-59 years
0.53%
0.005%
21,087
60-69 years
0.37%
0.021%
4,778
70-79 years
0.52%
0.094%
1,069
80-89
1.78%
0.469%
213
90 +
5.19%
1.608%
62
While some of the risk factors are higher in the viral hotspot of Quebec, it is still the case that under 80 years of age, your chances of dying from Covid 19 are better than 1 in 1000, and much better the younger you are.
Some time ago PM Trudeau floated the idea that pandemic shutdowns can’t be lifted until a vaccine is available. More recently, the lack of a vaccine is touted in the US as a reason for keeping schools closed and travel restrictions in place. What is this obsession with a vaccine as the savior whose healing powers we must await while hiding in isolation? As a previous post reprinted below explains, it is again a case of generals fighting a past war rather than the current one.
But let’s also be attentive to a bait and switch involving shifty use of words. A vaccine by definition works by training our immune system to recognize and resist a targeted pathogen. And it’s a long road to perfecting an agent which achieves that without doing harm to some or many individuals. Meanwhile Bill Gates is promoting something termed a “vaccine” which intends to modify our DNA to defend against SARS CV2. That is not like smallpox or polio vaccine. It is more like making humans a genetically modified organism (GMOs).
I have nothing against GMO plant inventions. As a British princess Anne reminded last month, the world benefited greatly from Canadian researchers who genetically modified rapeseed plants resulting in the nutritionally superior Canola vegetable oil. The “Green Revolution”, involving yellow rice relies on responsible use of GMO. But we drew the line at cloning humans, and the same goes for tinkering with people’s genetic codes.
[Comment: I am somewhat reassured by this statement from an article explaining DNA and RNA vaccines:
If there are ethical concerns in genetics, they might apply to techniques like human-gene editing, where a person’s DNA is altered to cut out a gene that might make you prone to a particular cancer. And those alterations can be passed on through generations. But that’s not the case with DNA vaccines. “They don’t alter a person’s DNA at all. They provide a temporary addition in a small number of cells,” says Gilbert. “DNA vaccines do not enter the genome.” Source: What’s the science on DNA and RNA vaccines?]
Let the race for real vaccines proceed, but we can’t count on a miracle finish any time soon, and it may even prove impossible for a coronavirus. Don’t forget SARS CV1 went away by itself before a vaccine could be deployed. If it turns out Sweden took the right strategy, SARS CV2 may also take its place beside other pathogens with which we learn to live. And in the meantime, many nations around the world are taking care of their citizens, saving lives with the HCQ+ treatment protocol.
Previous Post: The Virus Wars
The proverb is “Generals are always fighting the last war,” and its origin is uncertain. One possibility is a quote from Winston Churchill: “It is a joke in Britain to say that the War Office is always preparing for the last war.” 1948 Winston S. Churchill _The Second World War_ I (Boston: Houghton Mifflin, 1985) 426:
Konrad Lorenz demonstrated how imprinting works upon animal behavior, while military historians have reported how powerfully human social animals are influenced by the past and instilled lessons from others.
Austria – 20th century. Animal behaviourist Konrad Lorenz and mallard goslings
Which brings me to these reflections about the current WuHanFlu outbreak. The chart at the top summarizes our received epidemiological wisdom about the danger of viruses according to the dimensions of deadliness and contagiousness. As the diagram shows, extremely deadly viruses tend to kill their hosts too quickly to be transmitted widely. Conversely, a virus that spreads easily accomplishes that by slowly killing its hosts, perhaps even leaving them alive. The biggest threats are the germs that are lethal, but spread widely because the symptoms are slow to develop (longer incubation period).
Regarding the recent virus wars, consider these four (Source: Big Think. Excerpts in italics with my bolds)
SARS (started in Hong Kong in March 2003), Swine flu (started in Mexico in March 2009), Ebola (started in Western Africa in March 2014), and MERS (started in South Korea in May 2015).
The video below explains the last two impactful wars were against SARS and Swine Flu (HINI).
For the sake of comparison, the graphs for each epidemic are aligned so they all start together on Day One of each outbreak.
At first, Ebola is the scary one. Not only had it infected the most people after just one day, it had killed two thirds of those.
By comparison, SARS killed its first victim only after three days (out of 38 people infected).
By Day 10, SARS had overtaken Ebola as the most infectious of the outbreaks (264 vs. 145 patients), but the latter was ten times more lethal (91 dead from Ebola vs. 9 from SARS). At this time, the coronavirus had infected 39 people, killed none, and was still playing in the same minor league as the swine flu and MERS.
Day 20, and SARS cases are skyrocketing: 1,550 people are ill, 55 have died. That’s a death rate of 3.5%. Ebola has affected only 203 people by now, but killed 61.6% of them, a total of 125. Meanwhile, the coronavirus has taken Ebola’s second place, but is still far behind SARS (284 infected). At this time, the coronavirus has claimed the lives of just five people.
But now the coronavirus cases are exploding; by Day 30, the new virus has infected 7,816 people, killing 204. That’s far more infected than any other virus (SARS comes a distant second with 2,710 patients), and significantly more killed (Ebola, though still just 242 people ill, has killed 147, due to its high fatality rate). Meanwhile, MERS is stuck in triple digits, and the swine flu in double digits.
The swine flu numbers keep growing exponentially: by Day 80, they’ve passed 362,000 cases (and 1,770 deaths), far surpassing any of the other diseases.
Day 100: swine flu cases are approaching 1 million, deaths have surpassed 5,000. That’s far more than all the other diseases combined—they have merged into a single line at the bottom of the graph.
By Day 150, swine flu hit 5.2 million patients, with 25,400 people killed. By the time it was declared over, a year later, the outbreak would eventually have infected more than 60 million people and claimed the lives of almost 300,000.
Swine flu was caused by the H1N1 virus, which also caused the Spanish flu. That outbreak, in 1918/19, infected about 500 million people, or 1 in 3 people alive at that time. It killed at least 50 million people. It was the combination of extreme infectiousness and high fatality that made the Spanish flu such a global, lethal pandemic.
None of the other infectious diseases comes close to that combination. The swine flu, although more infectious than other diseases, was less infectious than the Spanish flu, and also less deadly (0.5%). Unlike COVID-19 or its fellow coronaviruses SARS and MERS, Ebola is not spread via airborne particles, but via contact with infected blood. That makes it hard to spread. Ironically, it may also be too lethal (39.6%) to spread very far. And COVID-19 itself, while relatively lethal (2.4%), is well below the deadliness of the Spanish flu, and does not seem to spread with the same ease.
As that history lesson shows, our pandemic generals have likely been preoccupied with three previous enemies: Spanish Flu, Swine Flu, and SARS. The first one served as the catastrophic defeat to be avoided, H1N1 as the victory achieved by deploying vaccine, and SARS as the coronavirus prototype. Naming the Wuhan virus SARS-CoV-2 (Severe acute respiratory syndrome coronavirus 2) predisposed tacticians and soldiers to fight against a viral pneumonia, and to expect air borne transmission as happened with SARS 1.
The battle plan was drawn up to protect the health care system against the deluge of victims coming to hospitals and ICUs. Flattening the curve of such cases was the strategy, and social distancing and personal immobility was imposed to that end. What has been the effect? For that there is an analysis from John Nolte What Terrible Coronavirus Models Tell Us About Global Warming Models H/T Joe D’Aleo Excerpts in italics with my bolds.
Let’s face it, the coronavirus models are terrible. Not just off, but way, way, way off in their predictions of a doomsday scenario that never arrived.
That’s not to say that over 20,000 dead Americans is not a heartbreaking reality. That’s not even to say that parts of the country should not have been shut down. But come on…
We shut the entire country down using the Institute for Health Metrics and Evaluation (IHME) models, and in doing so put 17 million (and counting) Americans out of work, shattered 17 million (and counting) lives, and… Well, take a look for yourself below.
That gigantic hump is the IHME’s April 1 prediction of coronavirus hospitalizations. The smaller humps way, way, waaaay below that are the IMHE’s predictions of coronavirus hospitalizations after they were revised just a few days later on April 5, 7, and 9.
The green line is the true number of hospitalizations, starting with the whole U.S., and into the states.
So why does this matter? And why are we looking at hospitalizations?
Well, remember, the whole reason for shutting down the economy was to ensure our healthcare system was not overloaded. And it should be noted that these expert models are based on full mitigation, based on what did indeed happen, which was basically a full shutdown of the economy by way of a lockdown. And these models are still horribly, terribly wrong.
Even if you believe the correct decision was made, that does not change how wildly wrong the coronavirus models were, are, and will almost certainly continue to be. That does not change the fact we shut down our entire economy based on incredibly flawed models.
Now I realize that the people who did the terribly flawed coronavirus models are not the same people who do the modeling for global cooling global warming climate change or whatever the hell these proven frauds are calling it today. But hear me out…
We’re still talking about “experts” our media and government grovel down to without question.
We’re still talking about models with the goal of destroying our way of life, our prosperity, our standard of living, and our individual freedoms to live our lives in whatever way we choose
We’re still talking about models with the goal of handing a tremendously scary amount of authority and power to a centralized government.
The coronavirus modeling was based on something real, on something happening at the time. The experts doing the coronavirus models had all kinds of data on which to make their assumptions. Not just reams and reams of scientific data based on previous pandemics, viruses, and human behavior; but also real-time data on the coronavirus itself from China, Italy, and other countries… And they still blew it. They still got it horribly wrong.
A health worker in protective gear waits to hand out self-testing kits in a parking lot of Rose Bowl Stadium in Pasadena, Calif., during the coronavirus outbreak, April 8, 2020. (Mario Anzuoni/Reuters)
What Went Wrong? California Provides a Clue
As the diagram at the top shows, WuHanFlu looked like an especially dangerous mix of deadly contagion. Thus California with its large population and extensive contact with China should be the US viral hot spot, and yet it isn’t. Maybe the contagion is real but the effects are milder than imagined.
Victor Davis Hanson writes at National Review Yes, California Remains Mysterious— Despite the Weaponization of the Debate. Excerpts in italics with my bolds.
How Many People Already Have COVID-19?
California is touchy, and yet still remains confused, about incomplete data showing that the 40-million-person state, as of Sunday, April 12, reportedly had 23,777 cases of residents who have tested posted for the COVID-19 illness. The number of infected by the 12th includes 674 deaths, resulting in a fatality rate of about 17 deaths per million of population. That is among the lowest rates of the larger American states (Texas has 10 deaths per million), and lower than almost all major European countries, (about half of Germany’s 36 deaths per million).
No doubt there are lots of questionable data in all such metrics. As a large state California has not been especially impressive in a per capita sense in testing its population (about 200,000 tests so far). Few of course believe that the denominator of cases based on test results represent the real number of those who have been or are infected.
There is the now another old debate over exactly how the U.S. defines death by the virus versus death because of the contributing factors of the virus to existing medical issues. Certainly, the methodology of coronavirus modeling is quite different from that of, say, the flu. The denominator of flu cases is almost always a modeled approximation, not a misleadingly precise number taken from only those who go to their doctors or emergency rooms and test positive for an influenza strain. And the numerator of deaths from the flu may be calibrated somewhat more conservatively than those currently listed as deaths from the coronavirus.
Nonetheless, the state’s population is fairly certain. And for now, the number of deaths by the virus is the least controversial of many of these data, suggesting that deaths per million of population might be a useful comparative number.
As I wrote in a recent NRO piece, the state on the eve of the epidemic seemed especially vulnerable given the large influx of visitors from China on direct flights to its major airports all fall and early winter until the January 31 ban (and sometime after). It ranks rather low in state comparisons of hospital beds, physicians, and nurses per capita. It suffers high rates of poverty, wide prevalence of state assistance, and medical challenges such as widespread diabetes.
This IHME projection is current as of April 14, at 12 p.m. ET, and will be updated periodically as the modelers input new data. The visualization shows the day each state may reach its peak between now and Aug. 4. The projected peak is when a state’s curve begins to show a consistent trend downward. To enlarge open image in new tab. Source: NPR
Certainly, both then and more recently, there have been a number of anecdotal accounts, media stories, and small isolated studies suggesting that more people than once thought, both here and abroad, have been infected with the virus and developed immunity, that the virus may have reached the West and the U.S. earlier than once or currently admitted by Chinese researchers — so, inter alia, California in theory could weather the epidemic with much less death and illness than earlier models of an eventual 25.5 million infected had suggested. Since then, a number of models, including Governor Newsom’s projection of 25.5 million infected Californians over an eight-week period, have been questioned. Controversy exists over exactly why models are being recalibrated downward. One explanation is that the shelter-in-space orders have been more successful than expected; others point to various flawed modeling assumptions.
Front-line physicians who see sick patients do not necessarily agree with researchers in the lab. For example, a Los Angeles Times story was widely picked up by other news outlets that quoted Dr. Jeff Smith, the chief executive of Santa Clara County. Smith reportedly now believes that the virus arrived in California much earlier than often cited, at least in early 2020:
The severity of flu season made health care professionals think that patients were suffering from influenza given the similarity of some of the symptoms. In reality, however, a handful of sick Californians that were going to the doctor earlier this year may have been among the first to be carrying the coronavirus. “The virus was freewheeling in our community and probably has been here for quite some time,” Smith, a physician, told county leaders in a recent briefing. The failure of authorities to detect the virus earlier has allowed it to spread unchecked in California and across the nation. “This wasn’t recognized because we were having a severe flu season. . . . Symptoms are very much like the flu. If you got a mild case of COVID, you didn’t really notice. You didn’t even go to the doctor. . . . The doctor maybe didn’t even do it because they presumed it was the flu.”
This is a reblog of the post at Sebastian Rushworth M.D. Health and medical information grounded in science. Excerpts in italics with my bolds.
Ok, I want to preface this article by stating that it is entirely anecdotal and based on my experience working as a doctor in the emergency room of one of the big hospitals in Stockholm, Sweden, and of living as a citizen in Sweden. As many people know, Sweden is perhaps the country that has taken the most relaxed attitude of any towards the covid pandemic. Unlike other countries, Sweden never went in to complete lockdown. Non-essential businesses have remained open, people have continued to go to cafés and restaurants, children have remained in school, and very few people have bothered with face masks in public.
Covid hit Stockholm like a storm in mid-March. One day I was seeing people with appendicitis and kidney stones, the usual things you see in the emergency room. The next day all those patients were gone and the only thing coming in to the hospital was covid. Practically everyone who was tested had covid, regardless of what the presenting symptom was. People came in with a nose bleed and they had covid. They came in with stomach pain and they had covid.
Then, after a few months, all the covid patients disappeared. It is now four months since the start of the pandemic, and I haven’t seen a single covid patient in over a month. When I do test someone because they have a cough or a fever, the test invariably comes back negative. At the peak three months back, a hundred people were dying a day of covid in Sweden, a country with a population of ten million. We are now down to around five people dying per day in the whole country, and that number continues to drop. Since people generally die around three weeks after infection, that means virtually no-one is getting infected any more. If we assume around 0.5 percent of those infected die (which I think is very generous, more on that later), then that means that three weeks back 1,000 people were getting infected per day in the whole country, which works out to a daily risk per person of getting infected of 1 in 10,000, which is miniscule. And remember, the risk of dying is at the very most 1 in 200 if you actually do get infected. And that was three weeks ago.
Basically, covid is in all practical senses over and done with in Sweden. After four months.
In total covid has killed under 6,000 people in a country of ten million. A country with an annual death rate of around 100,000 people. Considering that 70% of those who have died of covid are over 80 years old, quite a few of those 6,000 would have died this year anyway. That makes covid a mere blip in terms of its effect on mortality.
That is why it is nonsensical to compare covid to other major pandemics, like the 1918 pandemic that killed tens of millions of people. Covid will never even come close to those numbers. And yet many countries have shut down their entire economies, stopped children going to school, and made large portions of their population unemployed in order to deal with this disease.
The media have been proclaiming that only a small percentage of the population have antibodies, and therefore it is impossible that herd immunity has developed. Well, if herd immunity hasn’t developed, where are all the sick people? Why has the rate of infection dropped so precipitously? Considering that most people in Sweden are leading their lives normally now, not socially distancing, not wearing masks, there should still be high rates of infection.
The reason we test for antibodies is because it is easy and cheap. Antibodies are in fact not the body’s main defence against virus infections. T-cells are. But T-cells are harder to measure than antibodies, so we don’t really do it clinically. It is quite possible to have T-cells that are specific for covid and thereby make you immune to the disease, without having any antibodies. Personally, I think this is what has happened. Everybody who works in the emergency room where I work has had the antibody test. Very few actually have antibodies. This is in spite of being exposed to huge numbers of infected people, including at the beginning of the pandemic, before we realized how widespread covid was, when no-one was wearing protective equipment.
I am not denying that covid is awful for the people who do get really sick or for the families of the people who die, just as it is awful for the families of people who die of cancer, or influenza, or an opioid overdose.
But the size of the response in most of the world (not including Sweden) has been totally disproportionate to the size of the threat.
Sweden ripped the metaphorical band-aid off quickly and got the epidemic over and done with in a short amount of time, while the rest of the world has chosen to try to peel the band-aid off slowly. At present that means Sweden has one of the highest total death rates in the world. But covid is over in Sweden. People have gone back to their normal lives and barely anyone is getting infected any more. I am willing to bet that the countries that have shut down completely will see rates spike when they open up. If that is the case, then there won’t have been any point in shutting down in the first place, because all those countries are going to end up with the same number of dead at the end of the day anyway. Shutting down completely in order to decrease the total number of deaths only makes sense if you are willing to stay shut down until a vaccine is available. That could take years. No country is willing to wait that long.
Covid has at present killed less than 6000 in Sweden. It is very unlikely that the number of dead will go above 7,000. An average influenza year in Sweden, 700 people die of influenza. Does that mean covid is ten times worse than influenza? No, because influenza has been around for centuries while covid is completely new. In an average influenza year most people already have some level of immunity because they’ve been infected with a similar strain previously, or because they’re vaccinated. So it is quite possible, in fact likely, that the case fatality rate for covid is the same as for influenza, or only slightly higher, and the entire difference we have seen is due to the complete lack of any immunity in the population at the start of this pandemic.
This conclusion makes sense of the Swedish fatality numbers – if we’ve reached a point where there is hardly any active infection going on any more in Sweden in spite of the fact that there is barely any social distancing happening then that means at least 50% of the population has been infected already and have developed immunity, which is five million people. This number is perfectly reasonable if we assume a reproductive number for the virus of two: If each person infects two new, with a five day period between being infected and infecting others, and you start out with just one infected person in the country, then you will reach a point where several million are infected in just four months.
If only 6000 are dead out of five million infected, that works out to a case fatality rate of 0.12 percent, roughly the same as regular old influenza, which no-one is the least bit frightened of, and for which we don’t shut down our societies.
The map shows that in Canada 8979 deaths have been attributed to Covid19, meaning people who died having tested positive for SARS CV2 virus. This number accumulated over a period of 204 days starting January 31. The daily death rate reached a peak of 177 on May 6, 2020, and is down to 5 as of yesterday. More details on this below, but first the summary picture. (Note: 2019 is the latest demographic report)
Canada Pop
Ann Deaths
Daily Deaths
Risk per Person
2019
37589262
330786
906
0.8800%
Covid 2020
37589262
8979
44
0.0239%
Over the epidemic months, the average Covid daily death rate amounted to 5% of the All Causes death rate. During this time a Canadian had an average risk of 1 in 5000 of dying with SARS CV2 versus a 1 in 114 chance of dying regardless of that infection. As shown later below the risk varied greatly with age, much lower for younger, healthier people.
Background Updated from Previous Post
In reporting on Covid19 pandemic, governments have provided information intended to frighten the public into compliance with orders constraining freedom of movement and activity. For example, the above map of the Canadian experience is all cumulative, and the curve will continue upward as long as cases can be found and deaths attributed. As shown below, we can work around this myopia by calculating the daily differentials, and then averaging newly reported cases and deaths by seven days to smooth out lumps in the data processing by institutions.
A second major deficiency is lack of reporting of recoveries, including people infected and not requiring hospitalization or, in many cases, without professional diagnosis or treatment. The only recoveries presently to be found are limited statistics on patients released from hospital. The only way to get at the scale of recoveries is to subtract deaths from cases, considering survivors to be in recovery or cured. Comparing such numbers involves the delay between infection, symptoms and death. Herein lies another issue of terminology: a positive test for the SARS CV2 virus is reported as a case of the disease COVID19. In fact, an unknown number of people have been infected without symptoms, and many with very mild discomfort.
August 7 in the UK it was reported (here) that around 10% of coronavirus deaths recorded in England – almost 4,200 – could be wiped from official records due to an error in counting. Last month, Health Secretary Matt Hancock ordered a review into the way the daily death count was calculated in England citing a possible ‘statistical flaw’. Academics found that Public Health England’s statistics included everyone who had died after testing positive – even if the death occurred naturally or in a freak accident, and after the person had recovered from the virus. Numbers will now be reconfigured, counting deaths if a person died within 28 days of testing positive much like Scotland and Northern Ireland…
Professor Heneghan, director of the Centre for Evidence-Based Medicine at Oxford University, who first noticed the error, told the Sun: ‘It is a sensible decision. There is no point attributing deaths to Covid-19 28 days after infection…
For this discussion let’s assume that anyone reported as dying from COVD19 tested positive for the virus at some point prior. From the reasoning above let us assume that 28 days after testing positive for the virus, survivors can be considered recoveries.
Recoveries are calculated as cases minus deaths with a lag of 28 days. Daily cases and deaths are averages of the seven days ending on the stated date. Recoveries are # of cases from 28 days earlier minus # of daily deaths on the stated date. Since both testing and reports of Covid deaths were sketchy in the beginning, this graph begins with daily deaths as of April 24, 2020 compared to cases reported on March 27, 2020.
The line shows the Positivity metric for Canada starting at nearly 8% for new cases April 24, 2020. That is, for the 7 day period ending April 24, there were a daily average of 21,772 tests and 1715 new cases reported. Since then the rate of new cases has dropped down, now holding steady at ~1% since mid-June. Yesterday, the daily average number of tests was 43,612 with 375 new cases. So despite double the testing, the positivity rate is not climbing. Another view of the data is shown below.
The scale of testing has increased and has now reached nearly 50,000 a day, while positive tests (cases) are hovering at 1% positivity. The shape of the recovery curve resembles the case curve lagged by 28 days, since death rates are a small portion of cases. The recovery rate has grown from 83% to 98% steady over the last 2 weeks. This approximation surely understates the number of those infected with SAR CV2 who are healthy afterwards, since antibody studies show infection rates multiples higher than confirmed positive tests (8 times higher in Canada). In absolute terms, cases are now down to 375 a day and deaths 5 a day, while estimates of recoveries are 285 a day.
Summary of Canada Covid Epidemic
It took a lot of work, but I was able to produce something akin to the Dutch advice to their citizens.
The media and governmental reports focus on total accumulated numbers which are big enough to scare people to do as they are told. In the absence of contextual comparisons, citizens have difficulty answering the main (perhaps only) question on their minds: What are my chances of catching Covid19 and dying from it?
A previous post reported that the Netherlands parliament was provided with the type of guidance everyone wants to see.
The table presents only those cases with a full clinical documentation, which included some 2194 deaths compared to the 5842 total reported. The numbers show that under 60 years old, few adults and almost no children have anything to fear.
Update May 20, 2020
It is really quite difficult to find cases and deaths broken down by age groups. For Canadian national statistics, I resorted to a report from Ontario to get the age distributions, since that province provides 69% of the cases outside of Quebec and 87% of the deaths. Applying those proportions across Canada results in this table. For Canada as a whole nation:
Age
Risk of Test +
Risk of Death
Population per 1 CV death
<20
0.05%
None
NA
20-39
0.20%
0.000%
431817
40-59
0.25%
0.002%
42273
60-79
0.20%
0.020%
4984
80+
0.76%
0.251%
398
In the worst case, if you are a Canadian aged more than 80 years, you have a 1 in 400 chance of dying from Covid19. If you are 60 to 80 years old, your odds are 1 in 5000. Younger than that, it’s only slightly higher than winning (or in this case, losing the lottery).
As noted above Quebec provides the bulk of cases and deaths in Canada, and also reports age distribution more precisely, The numbers in the table below show risks for Quebecers.
Age
Risk of Test +
Risk of Death
Population per 1 CV death
0-9 yrs
0.13%
0
NA
10-19 yrs
0.21%
0
NA
20-29 yrs
0.50%
0.000%
289,647
30-39
0.51%
0.001%
152,009
40-49 years
0.63%
0.001%
73,342
50-59 years
0.53%
0.005%
21,087
60-69 years
0.37%
0.021%
4,778
70-79 years
0.52%
0.094%
1,069
80-89
1.78%
0.469%
213
90 +
5.19%
1.608%
62
While some of the risk factors are higher in the viral hotspot of Quebec, it is still the case that under 80 years of age, your chances of dying from Covid 19 are better than 1 in 1000, and much better the younger you are.
After examples of the media disinformation campaign, Steven provides a brief recounting of what has transpired over the last half year pandemic.
So what is the real story on hydroxychloroquine? Here, briefly, is what we know:
When the COVID-19 pandemic began, a search was made for suitable antiviral therapies to use as treatment until a vaccine could be produced. One drug, hydroxychloroquine, was found to be the most effective and safe for use against the virus. Federal funds were used for clinical trials of it, but there was no guidance from Dr. Anthony Fauci or the NIH Treatment Guidelines Panel on what role the drug would play in the national pandemic response. Fauci seemed to be unaware that there actually was a national pandemic plan for respiratory viruses.
Following a careful regimen developed by doctors in France, some knowledgeable practicing U.S. physicians began prescribing hydroxychloroquine to patients still in the early phase of COVID infection. Its effects seemed dramatic. Patients still became sick, but for the most part they avoided hospitalization. In contrast — and in error — the NIH-funded studies somehow became focused on giving hydroxychloroquine to late-presenting hospitalized patients. This was in spite of the fact that unlike the drug’s early use in ambulatory patients, there was no real data to support the drug’s use in more severe hospitalized patients.
By April, it was clear that roughly seven days from the time of the first onset of symptoms, a COVID-19 infection could sometimes progress into a more radical late phase of severe disease with inflammation of the blood vessels in the body and immune system over-reactions. Many patients developed blood clots in their lungs and needed mechanical ventilation. Some needed kidney dialysis. In light of this pathological carnage, no antiviral drug could be expected to show much of an effect during this severe second stage of COVID.
On April 6, 2020, an international team of medical experts published an extensive study of hydroxychloroquine in more than 130,000 patients with connective tissue disorders. They reaffirmed that hydroxychloroquine was a safe drug with no serious side effects. The drug could safely be given to pregnant women and breast-feeding mothers. Consequently, countries such as China, Turkey, South Korea, India, Morocco, Algeria, and others began to use hydroxychloroquine widely and early in their national pandemic response. Doctors overseas were safely prescribing the drug based on clinical signs and symptoms because widespread testing was not available.
However, the NIH promoted a much different strategy for the United States. The “Fauci Strategy” was to keep early infected patients quarantinedat home without treatment until they developed a shortness of breath and had to be admitted to a hospital. Then they would they be given hydroxychloroquine. The Food and Drug Administration cluelessly agreed to this doctrine and it stated in its hydroxychloroquine Emergency Use Authorization (EUA) that “hospitalized patients were likely to have a greater prospect of benefit (compared to ambulatory patients with mild illness).”
In reality just the opposite was true. This was a tragic mistake by Fauci and FDA Commissioner Dr. Stephen Hahn and it was a mistake that would cost the lives of thousands of Americans in the days to come.
At the same time, accumulating data showed remarkable results if hydroxychloroquine were given to patients early, during a seven-day window from the time of first symptom onset. If given during this window, most infections did not progress into the severe, lethal second stage of the disease. Patients still got sick, but they avoided hospitalization or the later transfer to an intensive care unit. In mid-April a high-level memo was sent to the FDA alerting them to the fact that the best use for hydroxychloroquine was for its early use in still ambulatory COVID patients. These patients were quarantined at home but were not short of breath and did not yet require supplemental oxygen and hospitalization.
Failing to understand that COVID-19 could be a two-stage disease process, the FDA ignored the memo and, as previously mentioned, it withdrew its EUA for hydroxychloroquine based on flawed studies and clinical trials that were applicable only to late-stage COVID patients.
By now, however, some countries had already implemented early, aggressive, outpatient community treatment with hydroxychloroquine and within weeks were able to minimize their COVID deaths and bring their national pandemic under some degree of control.
In countries such as Great Britain and the United States, where the “Fauci-Hahn Strategy” was followed, there was a much higher death rate and an ever-increasing number of cases. COVID patients in the U.S. would continue to be quarantined at home and left untreated until they developed shortness of breath. Then they would be admitted to the hospital and given hydroxychloroquine outside the narrow window for the drug’s maximum effectiveness.
In further contrast, countries that started out with the “Fauci-Hahn Doctrine” and then later shifted their policy towards aggressive outpatient hydroxychloroquine use, after a brief lag period also saw a stunning rapid reduction in COVID mortality and hospital admissions.
Finally, several nations that had started using an aggressive early-use outpatient policy for hydroxychloroquine, including France and Switzerland, stopped this practice when the WHO temporarily withdrew its support for the drug. Five days after the publication of the fake Lancet study and the resulting media onslaught, Swiss politicians banned hydroxychloroquine use in the country from May 27 until June 11, when it was quickly reinstated.
The consequences of suddenly stopping hydroxychloroquine can be seen by examining a graph of the Case Fatality Ratio Index (nrCFR) for Switzerland. This is derived by dividing the number of daily new COVID fatalities by the new cases resolved over a period with a seven-day moving average. Looking at the evolution curve of the CFR it can be seen that during the weeks preceding the ban on hydroxychloroquine, the nrCFR index fluctuated between 3% and 5%.
Following a lag of 13 days after stopping outpatient hydroxychloroquine use, the country’s COVID-19 deaths increased four-fold and the nrCFR index stayed elevated at the highest level it had been since early in the COVID pandemic, oscillating at over 10%-15%. Early outpatient hydroxychloroquine was restarted June 11 but the four-fold “wave of excess lethality” lasted until June 22, after which the nrCFR rapidly returned to its background value.
Here in our country, Fauci continued to ignore the ever accumulating and remarkable early-use data on hydroxychloroquine and he became focused on a new antiviral compound named remdesivir. This was an experimental drug that had to be given intravenously every day for five days. It was never suitable for major widespread outpatient or at-home use as part of a national pandemic plan. We now know now that remdesivir has no effect on overall COVID patient mortality and it costs thousands of dollars per patient.
Hydroxychloroquine, by contrast, costs 60 cents a tablet, it can be taken at home, it fits in with the national pandemic plan for respiratory viruses, and a course of therapy simply requires swallowing three tablets in the first 24 hours followed by one tablet every 12 hours for five days.
There are now 53 studies that show positive results of hydroxychloroquine in COVID infections. There are 14 global studies that show neutral or negative results — and 10 of them were of patients in very late stages of COVID-19, where no antiviral drug can be expected to have much effect. Of the remaining four studies, two come from the same University of Minnesota author. The other two are from the faulty Brazil paper, which should be retracted, and the fake Lancet paper, which was.
Millions of people are taking or have taken hydroxychloroquine in nations that have managed to get their national pandemic under some degree of control. Two recent, large, early-use clinical trials have been conducted by the Henry Ford Health System and at Mount Sinai showing a 51% and 47% lower mortality, respectively, in hospitalized patients given hydroxychloroquine. A recent study from Spain published on July 29, two days before Margaret Sullivan’s strafing of “fringe doctors,” shows a 66% reduction in COVID mortality in patients taking hydroxychloroquine. No serious side effects were reported in these studies and no epidemic of heartbeat abnormalities.
This is ground-shaking news. Why is it not being widely reported? Why is the American media trying to run the U.S. pandemic response with its own misinformation?
Steven Hatfill is a veteran virologist who helped establish the Rapid Hemorrhagic Fever Response Teams for the National Medical Disaster Unit in Kenya, Africa. He is an adjunct assistant professor in two departments at the George Washington University Medical Center where he teaches mass casualty medicine. He is principle author of the prophetic book “Three Seconds Until Midnight — Preparing for the Next Pandemic,” published by Amazon in 2019.






 Norman Doige writes in The Tablet
Norman Doige writes in The Tablet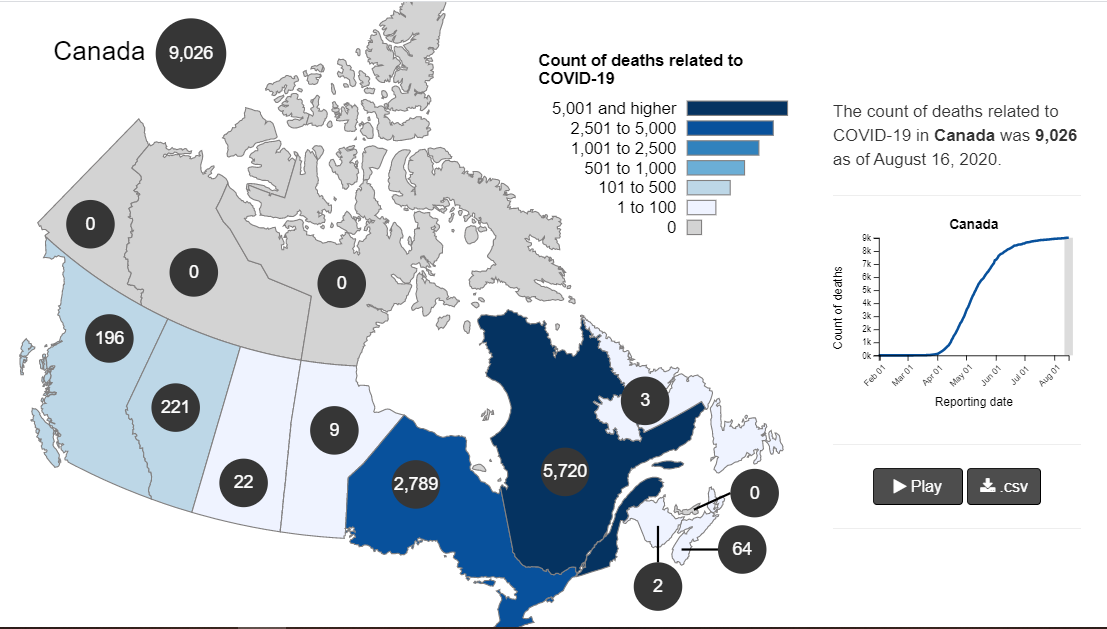
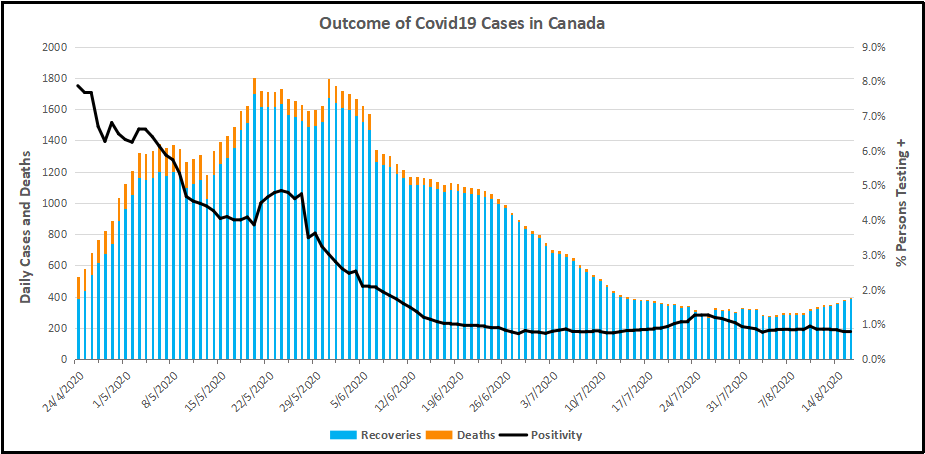
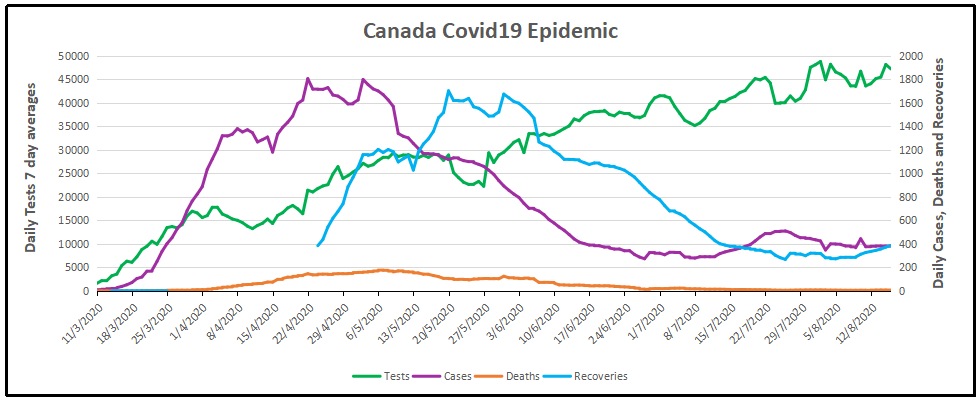

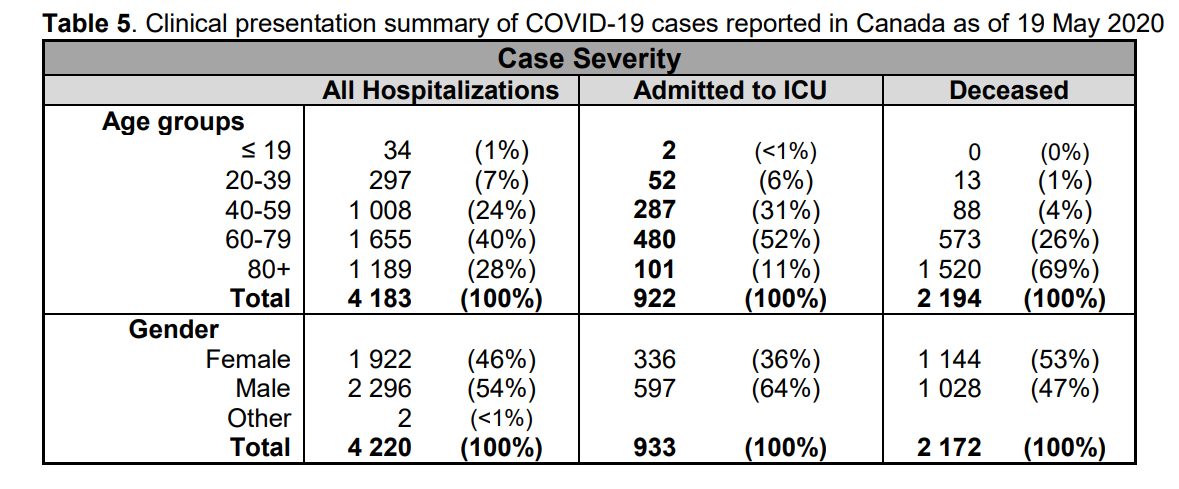

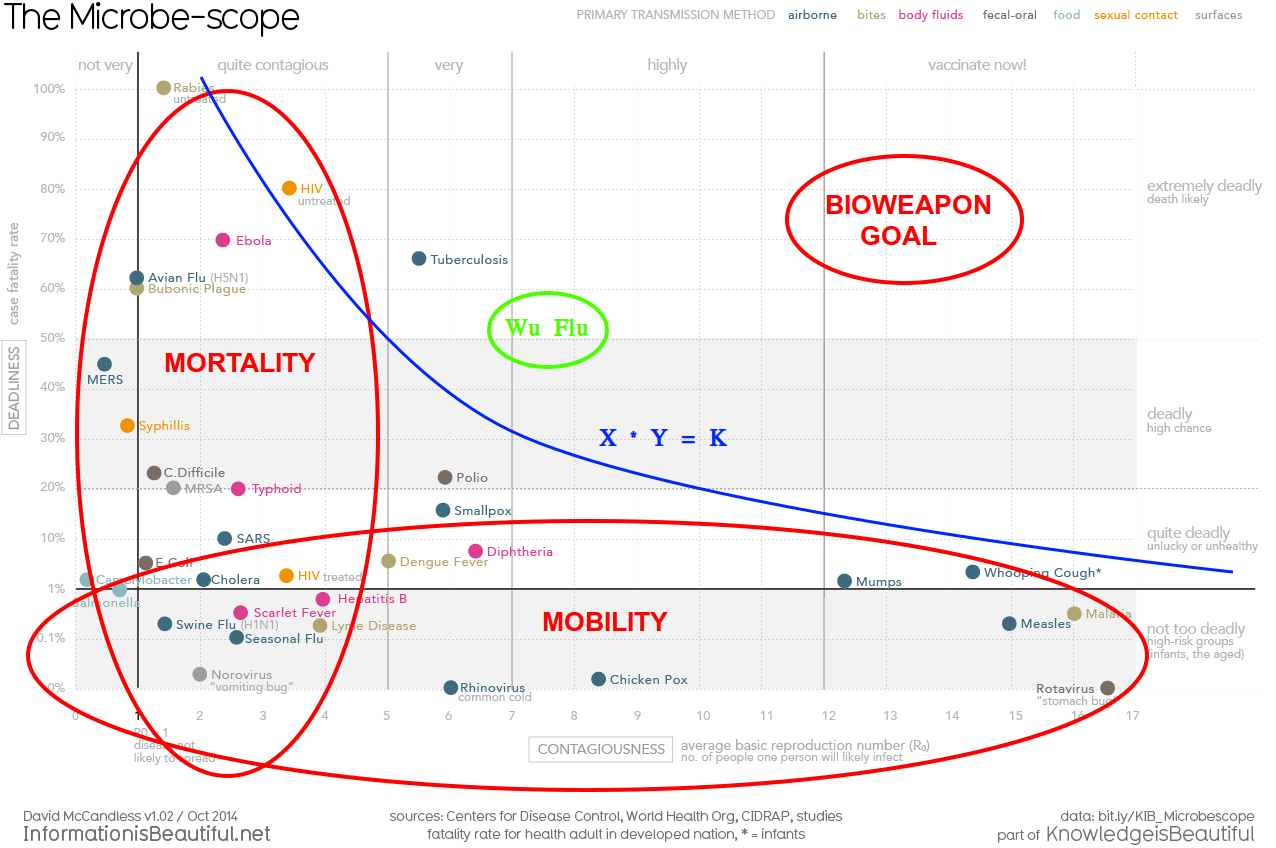


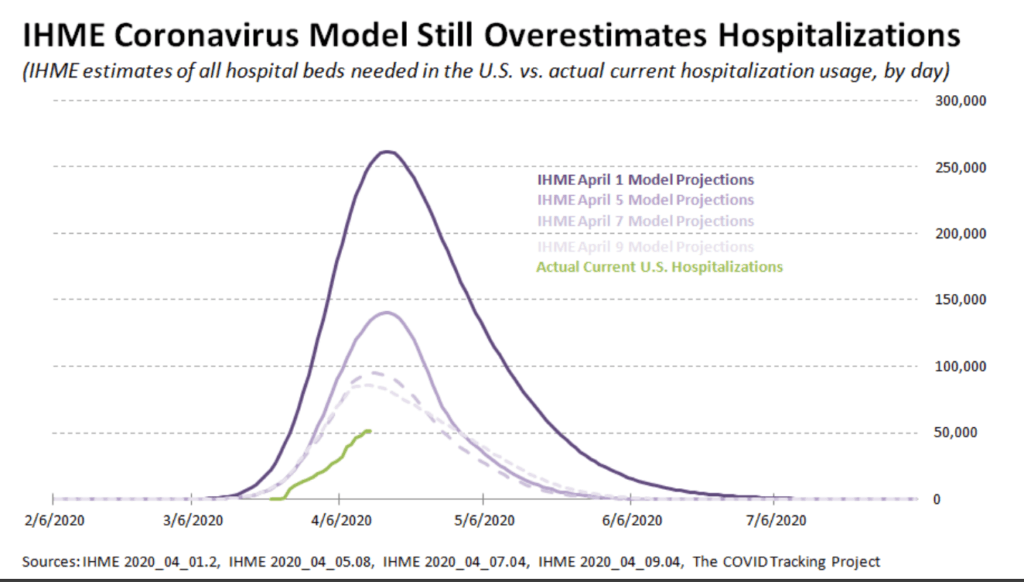
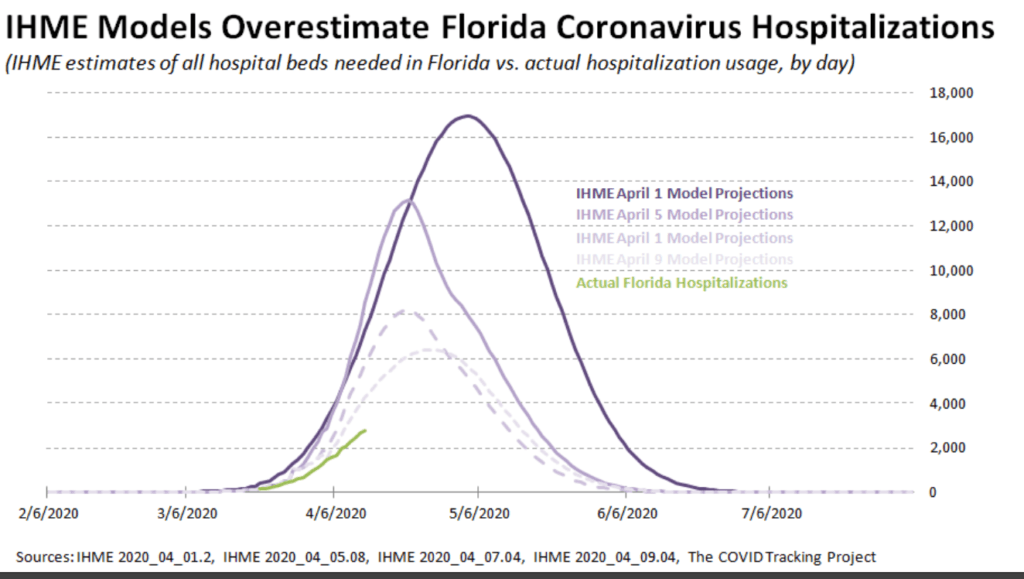
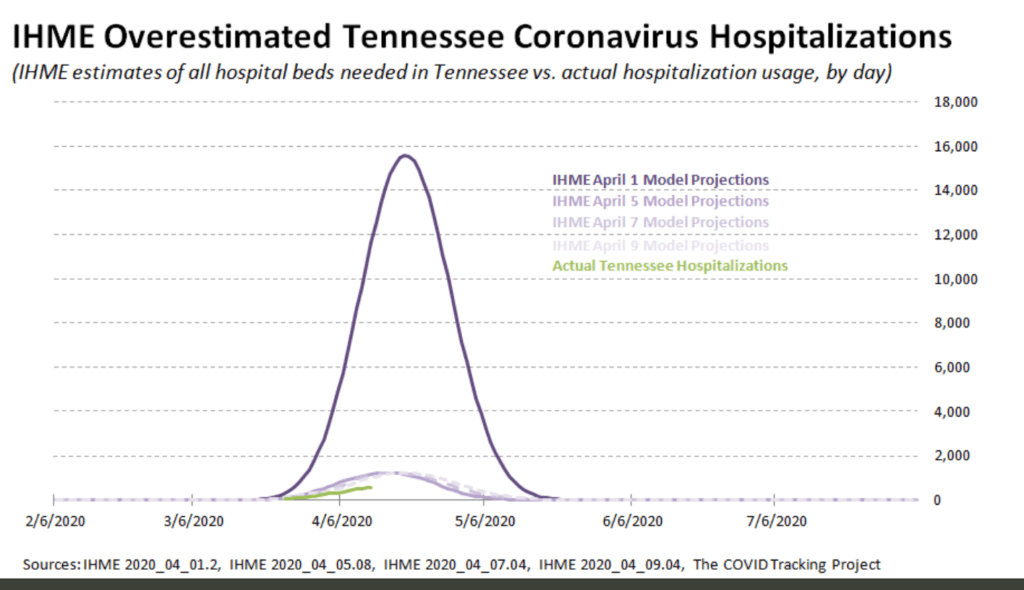

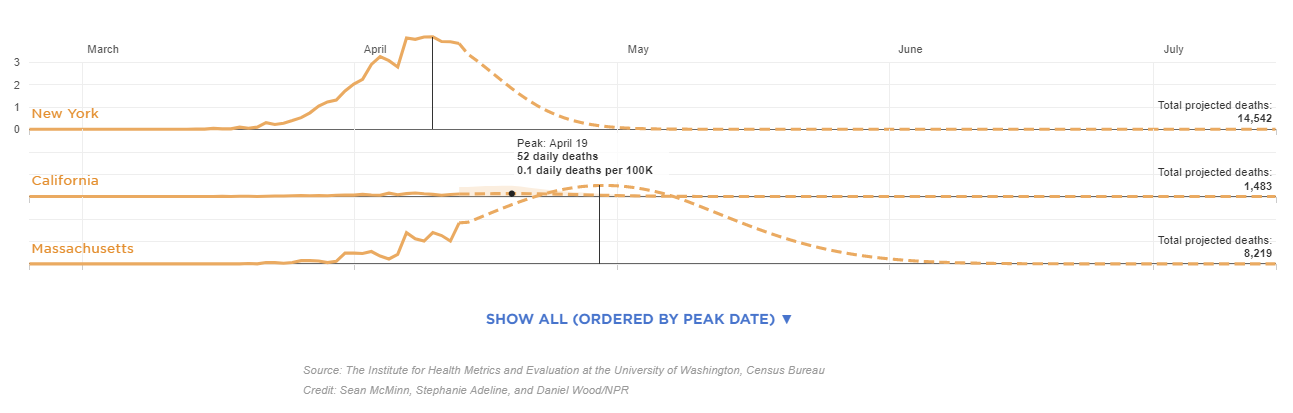
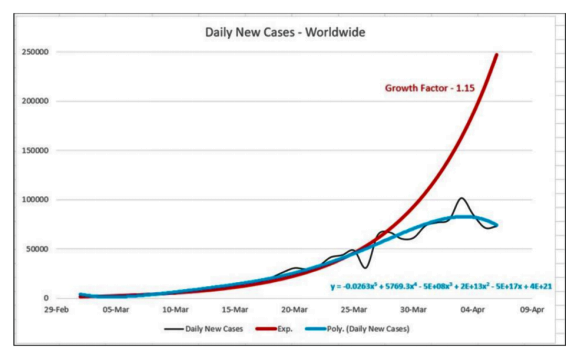













{kind=link}