The Ivermectin True Story in 15 minutes
 Toby Young writes at Spectator How science became politicized. Excerpts in italics with my bolds and added images.
Toby Young writes at Spectator How science became politicized. Excerpts in italics with my bolds and added images.
New rules from a leading journal do not bode well
Here’s a paradox. Over the past two-and-a-half years, a cadre of senior politicians and their “expert” advisors across the world have successfully promoted a series of controversial public policies by claiming they’re based on “the science” rather than a particular moral or ideological vision. I’m thinking of lockdowns and net zero in particular. Yet at the same time, this group has engaged in behavior that has undermined public confidence in science.
Why appeal to the authority of science to win support for a series of politically contentious policies — and then diminish its authority?
Take Anthony Fauci, for instance, who recently announced he’s stepping down as chief medical advisor to Joe Biden. Even though he once claimed to “represent science” in the eyes of the American people:
♦ he misled them about the likely duration of the lockdowns (“fifteen days to slow the spread”),
♦ overstated the efficacy of the Covid vaccines when they were first rolled out,
♦ refused to countenance the possibility that Covid-19 leaked from the Wuhan Institute of Virology
♦ it later emerged that the National Institute of Allergy and Infectious Diseases, under his leadership, had given a grant to the EcoHealth Alliance, which helped fund “gain-of-function” research at the Chinese lab,
♦ and he conspired with other prominent scientists, such as Francis Collins, to besmirch the authors of the Great Barrington Declaration (“There needs to be a quick and devastating published takedown of its premises,” Collins told Fauci in an email).
A recent editorial in the Wall Street Journal concluded: “His legacy will be that millions of Americans will never trust government health experts in the same way again.”
Another case in point is a recent editorial in Nature Human Behaviour, one of several journals in the Nature Research stable, the world’s pre-eminent publisher of scientific research. “Although academic freedom is fundamental, it is not unbounded,” it begins, and then proceeds to set out rules that future academic papers will have to comply with in addition to meeting all the usual standards for publication, e.g. peer review. It says the journal won’t publish articles that might cause “potential harms” (even “inadvertently”) to individuals or groups that are most vulnerable to “racism, sexism, ableism or homophobia.” “Academic content that undermines the dignity or rights of specific groups; assumes that a human group is superior or inferior over another simply because of a social characteristic; includes hate speech or denigrating images; or promotes privileged, exclusionary perspectives raises ethics concerns that may require revisions or supersede the value of publication,” it says.
It should be obvious that far from being politically neutral, these rules embody a particular ideology and in future the truthfulness of a scientific finding will be subordinate to this perspective.
To see this, you just need to do a simple thought experiment, as Bo Winegard has done in Quillette. Imagine, he says, if this editorial had been written by political conservatives who announced that “any research promoting (even ‘inadvertently’) promiscuous sex, the breakdown of the nuclear family, agnosticism and atheism, or the decline of the nation state, would be suppressed or rejected lest it inflict unspecified ‘harm’ on vaguely defined groups or individuals.” Those progressive scientists applauding Nature Human Behaviour would throw up their arms in horror and point out – correctly — that these rules are at odds with one of the foundational principles of science, which is to pursue the truth, wherever it may lead.
![]()
This editorial is a disaster from the point of view of closet ideologues who want to appeal to the authority of science to promote lockdowns and net zero, including, I suspect, its authors. After all, the reason rhetorical phrases like “the science” are supposed to win round those who are skeptical about these policies — conservatives, for the most part — is that they invoke a popular conception of scientists as politically neutral, disinterested “experts” who are basing their guidance on reason and evidence, uncontaminated by value judgments.
Yet here is a group of senior scientific gatekeepers announcing that the only knowledge that will count as “scientific” is that which promotes their agenda.
It’s as if they’re saying that scientific research unconstrained by this progressive straitjacket, i.e. science as conventionally understood, will yield results that are incompatible with their radical egalitarian agenda and so ought to be suppressed. In other words, “the science” is actually at odds with their political views.
How to explain this own goal? As I say, it’s a head-scratcher.

 Michael Fumento investigates The Myth — and Grift — of Long COVID in his American Spectator article. Excerpts in italics with my bolds and added images.
Michael Fumento investigates The Myth — and Grift — of Long COVID in his American Spectator article. Excerpts in italics with my bolds and added images.
Validating people’s fears is a lucrative business.
The would-be monkeypoxalypse isn’t panning out as some would like — no deaths have been reported outside of Africa — and apparently 99 percent of U.S. victims are gay men having sex with gay men.
And, while acute COVID-19 is still spinning off variants and Health and Human Services (HHS) has just extended the public health emergency, people are just plumb tired of hearing about it. But moving in to fill the clickbait quota is the so-called “long COVID” or “long-haul COVID.”
“Do I have Long COVID? As many as 23 million Americans want to know,
as more than 200 symptoms emerge.”
So begins a recent article in Fortune magazine. “It gets stranger,” the piece continues. “Among the 200-plus symptoms identified so far are ear numbness, a sensation of ‘brain on fire,’ erectile dysfunction, irregular menstrual periods, constipation, peeling skin, and double vision.” This is according to a study published a year ago in the British medical journal the Lancet, widely considered the world’s most prestigious medical journal. And, oh yes, “The study identified symptoms involving 10 major organ systems—and the body only has 11.”

If you haven’t recently suffered at least a dozen of these symptoms, it’s bad news for you. You’re dead.
We all know the expression “If it sounds too good to be true ….” Why is there no corollary that says, “If it sounds too bad …”? Do you have to be a genius’ genius, say Albert Einstein level, to recognize that over 200 symptoms in almost all major organ systems have no relationship, that this is just a constellation of symptoms — which has now grown so large that it cannot possibly count as a constellation anymore?
It’s essentially anything bad. The “search for causes and cures” for “long COVID” will never end, any more than we will ever find Bigfoot or the Loch Ness Monster.
Oh, and this is really important. Official definitions aside, in order to have “long COVID,”
there’s absolutely no need to ever have had acute COVID.
Obviously, some people who contract COVID do have long-term symptoms, as with the flu or other diseases that usually resolve fairly quickly but sometimes have lingering problems.
Yet, as I noted in my first “long COVID” article in The American Spectator last September:
The largest study so far of “long-haulers,” published by researchers at University College London in July, comprised nearly 4,000 subjects from over 56 countries. Participants were over the age of 18 and suffered from symptoms lasting at least 28 days. The researchers acknowledged merely in passing that in the study a mere 27% or 1020 of these “COVID long-haulers” had evidence of exposure to the SARS-CoV-2 virus. That’s whether antigen [during infection] or antibody [post-infection]. The only connection to COVID was the attestation of the sufferers. They “felt” they had COVID, regardless of evidence.
So about three-fourths of the participants don’t fit any of the above definitions. Yet that is the study that Fortune cites.
An August 2021 study of 3,151 British “long haulers” in Pragmatic and Observational Research found that only 17.2 percent were “test-confirmed positive.” A further 12 percent said they were told they had acute COVID, but no test was performed. And over 70 percent admitted it was merely self-diagnosis. An influential and scary article in the Atlantic reported some two-thirds of “long-hauler” patients had negative coronavirus antibody tests without making the obvious inference. An advocacy group study released in May 2020 by the curiously named “Patient-Led Research Collaborative” found that only “[a]bout a quarter of respondents (23.1%) tested positive for COVID-19” but “[i]n our analysis, we included all responses regardless of testing status.”
 And the game continues. No, not just with the popular clickbait media. With the vaunted “published, peer-reviewed” medical journals that have names most people don’t even understand, like Annals of Clinical and Translational Neurology. A May 2022 issue reports on a selected cohort of 100 “non-hospitalized COVID-19 ‘long haulers.’” Yet these included “50 laboratory-negative” people. Again, they didn’t just not test positive but rather had tested negative. But this time it was made clear they were included because they were negative!
And the game continues. No, not just with the popular clickbait media. With the vaunted “published, peer-reviewed” medical journals that have names most people don’t even understand, like Annals of Clinical and Translational Neurology. A May 2022 issue reports on a selected cohort of 100 “non-hospitalized COVID-19 ‘long haulers.’” Yet these included “50 laboratory-negative” people. Again, they didn’t just not test positive but rather had tested negative. But this time it was made clear they were included because they were negative!
They didn’t read the WHO, CDC, Mayo Clinic, etc., definitions?
Clearly they had. And rejected them. You see, “it has been advocated that a positive test for COVID-19 should not be a perquisite for diagnosis” (emphasis mine). As I noted in my original article, like so many faux diseases before it, such as the CDC-recognized “myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS),” so-called “long COVID” has been co-opted by advocacy groups whose main purpose is to engage in what’s called “beating up the numbers.” That is, making them seem greater. This has been going on since AIDS, when beginning around 1984 AIDS was converted from a disease overwhelmingly afflicting male homosexuals and intravenous drug abusers to “An Equal Opportunity Destroyer.”
The difference between AIDS and “long COVID” is that, at the time, you could play games regarding how people contracted the disease, but the definition of AIDS in the U.S. and Europe was quite fixed and absolutely required a positive HIV test. But if we do what “long COVID” advocates want and eliminate the need for a positive COVID test, then, given that absolutely everyone not only has had some of the ever-growing list of 200-plus symptoms but probably still does, we can literally say that everyone is suffering “long COVID.” Of course, that would be going a bit far, as when I saw extrapolations of AIDS cases to a point where people claimed more Americans would die of AIDS than there were Americans. So instead, we see the numbers pumped up to something that’s just on the edge of reason. Or maybe a bit beyond. The Atlantic tells us the U.S. has “at least 56 million long-COVID patients.” Or, as it says, “one for every six Americans.” Do we really believe that?
Disease advocacy groups, of which “long COVID” had at least 50 as of February of last year, have various motives. An obvious one is that more attention means more funding.
Removal of stigma is not universal, but special treatment is. And indeed, in a joint statement last year, HHS and the Department of Justice ruled that “long COVID can be a disability” under the Americans with Disabilities Act, thereby protecting alleged sufferers from “discrimination.” With allegedly over 200 symptoms, pretty much whatever you say your problem is can be protected. The range is broad enough to include demanding more time to take tests. Want a better chance at acing that exam? Claim to have “long COVID.” It does, however, require an “individualized assessment,” which is presumably as easy as calling up a list of alleged symptoms or, actually, just claiming virtually any symptoms.

Advocates also want to make a special exception for alleged sufferers to collect social security disability payments more quickly. As it stands, you don’t need a “long COVID” diagnosis to qualify if your symptoms are among those covered. But there’s a waiting period, and they want that shortened just for those who claim to have “long COVID.”
All that said, the Annals authors’ own data make the case that there’s no such thing as “long COVID.” Table 2 has three separate breakdowns. It kindly separates those who tested positive from those who tested negative, and then breaks them down further into neurologic and other symptoms upon first visit and then upon follow-up. And lo! — it turns out that time and again the ones who tested negative (and, even by the woke standards of the authors, are thereby more likely to never have had acute COVID) are worse off.
So, if nothing else, when you see an article in the popular media cite official or authoritative definitions of “long COVID” and then proceed to discuss what it may be, don’t let them mislead you into thinking they’re going by those definitions. Essentially, they’re going by whatever they think will keep you reading or by what they feel is the “right thing to do.”
But why would there be a difference between the positive and negative groups with the negatives worse off? Because those who actually have had COVID may be suffering extended symptoms from their disease. May. But those who never had COVID, but are convinced they have, are more likely to have psychological problems, and psychological problems are notoriously difficult to treat. Especially if ignored in favor of something else.
That’s why you haven’t seen terminology in this article such as “alleged sufferers.” Because if you think you’re sick, you’re sick. It’s just that, if you had negative tests for acute COVID, you almost certainly don’t have “long COVID.”
Mind, just as “long haulers” who test negative are different from those who test positive, “long haulers” generally have very little overlap with sufferers of acute COVID. While acute COVID is highly contagious and therefore virtually everyone is susceptible to contracting it (some people repeatedly), those who develop severe symptoms fit a very tight profile. Overwhelmingly they are older, with a plurality of deaths over age 80, and have several preconditions or comorbidities such as diabetes and untreated hypertension. According to the CDC, in the U.S. among acute COVID patients, non-Hispanic American blacks are slightly more likely to be diagnosed with the disease, almost three times as likely to be hospitalized, and are twice as likely to have died, compared with non-Hispanic whites.
But “long-haulers,” according to an appendix in the 2021 University College study, “belong to the middle and upper-middle income brackets, with 51.0% of participants in the USA earning more than $85,000/year and 22.5% earning more than $150,000/year.” They are overwhelmingly white and female. In fact, the demographics match pretty well to those diagnosed with the above-mentioned phantom illness, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), for which coincidentally there’s also no cure. The Veterans’ Department says: “[R]esearch suggests that women are 4X more likely to get [ME/CFS] than men. Statistics also show that people between ages 40 and 59 are most affected by the disorder.”

Mostly, as with so many other “syndromes,” these people suffer from depression. My interpretation? No, theirs. In the Annals study, the majority of the COVID-negative patients actually claimed depression as looming large among their symptoms, both upon initial visit and follow-up. Meanwhile, this being a journal of neurology, any symptom they list, such as shortness of breath, can be associated with depression and/or anxiety.
Even the mainstream media have observed the “long COVID” link to depression, as a Google search quickly shows. But they consistently put the cart before the horse. That is, they blame depression on “long COVID” rather than “long COVID” on depression. A typical headline: “How Long Haul COVID Takes a Toll on Your Mental Health.”
And, sadly, the worst thing you can do with depressives is to patronize them. You should tell them that they are suffering from depression and that it is a very real and serious disease (successful suicide has a 100 percent mortality rate), and then you should refer them to an expert who may be able to treat them.
You do not attribute their illness to something that doesn’t exist. That’s not only uncompassionate, it’s downright cruel. Yet, it’s also a great way to sell them snake oil to cure them.
But how many researchers have dared publish the clear reality? Precious few. Or at least few have succeeded; we have no idea what’s been rejected. It’s treated the same as was the case that said AIDS victims are overwhelmingly gay males and drug abusers, as the data clearly showed. I lost two jobs over that and was unemployable for two years. Likewise, did you know that monkeypox victims are 99 percent male and gay before you read it here?
A commentary last year in America’s most prestigious medical journal, the New England Journal of Medicine (NEJM), actually launched a preemptive strike against those who believe “long COVID” to be “likely to have a non-physiological origin.” The opinion piece, titled “Confronting Our Next National Health Disaster — Long-Haul Covid,” declares the authors to be aghast that “[s]ome commentators have characterized it as a mental illness.”
In late 2020, the godfather of America’s acute COVID hysteria, National Institute of Allergy and Infectious Disease (NIAID) Director Anthony Fauci, declared “long COVID” to be “quite real and quite extensive.” That’s the same Fauci who apparently got promoted to that position shortly after essentially kick-starting the “AIDS democratization” campaign in 1983 with an article in the prestigious Journal of the American Medical Association (JAMA), saying that there was evidence of casual transmission. This was long after it had been made clear it was a difficult-to-transmit disease of bodily fluids.

It’s also hardly insubstantial that Congress is paying bounties for discussing the will o’ the wisp, providing “$1.15 billion in funding over four years” for the National Institutes of Health (NIH) to support research. And if you think you’re going to get a grant by labeling it as something other than what the former head of NIH, the current acting director, Fauci, the NEJM, and the medical establishment in general has, hopefully you’re living in a state where smoking those mushrooms is legal.
Over a billion bucks is dedicated to the RECOVER program, under which, as of February,
66 hospitals and health systems had launched post-COVID clinics.
So it’s a massive gravy train. There’s much money in spotting Nessie and Bigfoot, less than nothing in denying their existence. In fact, the few who have published in medical journals suggesting it’s not a real disease have been pounded. There is precedent for this intimidation. My experience with AIDS, for example. Lost jobs, long-term unemployment, books banned.
But there’s also precedent with others and other diseases. About four years ago, Reuters ran a remarkable article called “Online activists are silencing us, scientists say,” regarding ME/CFS. It noted that researchers seeking answers to actual causes of the syndrome and bona fide treatments said they were abandoning the field because of bullying. “Of more than 20 leading research groups who were publishing treatment studies in high-quality journals 10 years ago,” one scientist said, “only one or two continue to do so.” Their sin was in positing psychological rather than organic explanations and, therefore, appropriate treatments. The campaign to have evidence-backed treatments discredited was “doing a terrible disservice to sufferers from this condition,” said another. He concluded, “Patients are the losers here.”
What Ronald E. Gots wrote of an alleged syndrome, multiple chemical sensitivities (MCS), in 1995 in the Journal of Toxicology holds equally true for “long COVID.” It’s “a dangerous diagnosis,” says the executive director of the Environmental Sensitivities Research Institute in Rockville, Maryland, a clearinghouse for scientific data. He continues:
[T]he diagnosis of MCS begins a downward spiral of fruitless treatments, culminating in withdrawal from society and condemning the sufferer to a life of misery and disability. This is a phenomenon in which the diagnosis is far more disabling than the symptoms.
It’s wickedly cruel! We need to really care about these people, not pretend that we do. We need to tell them they need help, that they quite possibly can be helped, but that, even if they tested positive for COVID, what they have is probably not COVID-related, and, if they tested negative, it almost certainly is not.
But don’t hold your breath waiting for an advocacy group or even the medical journal industry — and indeed it is an industry — to take that position. All the money, fame, and fortune are pointing in a different direction.

 Christopher Gage writes at his blog Oxford Sour The Cost of Folly Excerpts in italics with my bolds and added images.
Christopher Gage writes at his blog Oxford Sour The Cost of Folly Excerpts in italics with my bolds and added images.
Sociologists say one third of any society harbours a ‘latent authoritarianism.’ All they need is a little wink and a nudge from someone in a lab coat.
For such people, the pandemic was the glory days of a humdrum existence.
They were the winners. They studied the ever-changing rules, the more ridiculous the better. They pretended Sweden didn’t exist. They willed Florida to swamp herself in Covid deaths.
When such measures failed, they recanted with primitive fervour: ‘We didn’t lock down hard enough!’
The pandemic celebrated usually negative personality traits. High neuroticism combined with high agreeableness—the psychic soup of scolds and puritans—became the stuff of winners.
Back then, ten percent of people consistently told pollsters they’d lockdown indefinitely. A crazy poll in The Economist found forty percent wanted masks to remain; a quarter would shut down all nightclubs and casinos; another third craved socially-distanced theatres, pubs, and stadiums. A sizeable number wanted a 10 p.m. curfew! And they wanted all this regardless of Covid-19.
No doubt, the same people would now tell pollsters much different. The social currency of lockdown fanaticism has, like our money, eroded in value.

But they’re still there, and given the chance, they’ll fall in line when the conditions are right.
In his work, The True Believer, Eric Hoffer said that “by embracing a holy cause and dedicating their energies and substance to its advancement,” such people, “find a new life of purpose and meaning.”
To some, the pandemic was the great equaliser. Freedom to them is an ‘irksome burden’ and revealing of one’s shortcomings. As Hoffer said, they want freedom from freedom itself.

Why is it so many obey authority when coerced?
Social psychologist Stanley Milgram’s obedience experiments found that people obeyed either out of fear or out of a desire to fit in, even when obeying went against their better judgements.
In Milgram’s classic study, sixty-five percent were willing to administer a fatal dose of electricity to a fellow human being, provided an authority figure told them to do so. Participants were told the experiment would study the effects of punishment on learning. The ‘learner’ (an actor) was rigged up to electrodes.
The ‘teacher’ (an unknowing participant) was instructed to ask the learner questions, and zap the learner for any wrong answers, increasing the severity of the shock for each wrong answer. The shock generator was marked from 15 volts (a slight shock) to 450 volts (Danger! Severe shock.) The final shock was marked: ‘XXXX.’
The actor would provide the wrong answers on purpose. And dial up the volume of his complaints as the shocks got worse. A slight shock elicited a grunt. He’d scream in agony at 285 volts. Further up the scale, he’d complain of heart pain. At 330 volts: total silence.
When the teacher hesitated, the experimenter would pressure him to keep going: From, ‘please continue,’ to ‘the experiment requires that you continue,’ to ‘You have no choice but to continue.’
One teacher who begged to end the experiment was told he must continue. He went on, repeating to himself: “It’s got to go on. It’s got to go on.”
Milgram found that over two-thirds of ordinary people, when ordered to by an authority figure, would administer a fatal 450v shock to an innocent human being.
Another study found many will change their beliefs to fit in. Solomon Asch asked participants to match one line with three other lines. Two lines were of obviously different lengths, and one line was of obviously matching length.
Without actors present, 99 percent of participants answered correctly. When surrounded by actors claiming a shorter or longer line was actually the matching line, the result was much different. A full 37 percent of participants would change their mind to agree with the others, despite the correct answer being childishly obvious.
Asch said of the results, “That intelligent, well-meaning, young people are willing to call white, black is a matter of concern.”
And don’t we know it.
Freedom is not our default state. Our default state is of safety and suspicion. The free society is an aberration. That’s something we tend to forget.
Postscript: Clive James once said: ‘The problem with Australians is not that so many of them are descended from convicts but that so many are descended from prison officers.’


My title concerning mRNA vaccines is a play on the Animal Farm slogan. It’s prompted by research reports looking for answers why highly vaccinated populations like those in Europe and North America experience continuing Omicron infections, while other places like Africa do not. The surprising finding is summarized at the end of the report. While two vax shots do not prevent future infections, they do protect against serious illness from the virus, and thus benefit the persons. But the data suggest that additional booster shots are counter-productive by diminishing the immune system response to further viral exposure.
The paper published in Science is Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure.
A long-term study of healthcare workers in the United Kingdom has allowed their history of infection and vaccination to be traced precisely. Reynolds et al. found some unexpected immune-damping effects caused by infection with a heterologous variant to the latest wave of infection by the Omicron/Pango lineage B.1.1.529. The authors found that Omicron infection boosted immune responses to all other variants, but responses to Omicron itself were muted. Infection with the Alpha variant provided weaker boosting for Omicron-specific responses. Furthermore, Omicron infection after previous Wuhan Hu-1 infection failed to boost neutralizing antibody and T cell responses against Omicron, revealing a profound imprinting effect and explaining why frequent reinfections occur.
Vaccine boosting results in distinct, imprinted patterns of hybrid immunity with different combinations of SARS-CoV-2 infection and vaccination. Immune protection is boosted by B.1.1.529 (Omicron) infection in the triple-vaccinated, previously infection-naïve individuals, but this boosting is lost with prior Wuhan Hu-1 imprinting. This “hybrid immune damping” indicates substantial subversion of immune recognition and differential modulation through immune imprinting and may be the reason why the B.1.1.529 (Omicron) wave has been characterized by breakthrough infection and frequent reinfection with relatively preserved protection against severe disease in triple-vaccinated individuals.
The report by Jennifer Margulis and Joe Wang from Epoch Times is New Science Shows Vaccines Help Omicron Spread: Peer-Reviewed Study. Excerpts in italics with my bolds.
A team of 19 scientists from the United Kingdom have published new research that helps explain why countries with the highest vaccination rates are experiencing the highest numbers of what they call “breakthrough infections,” as well as reinfection with other variants of COVID-19.
This research article, published on June 14, 2022 in the peer-reviewed journal Science, has been downloaded nearly 277,500 times in less than two months. That is very unusual for a densely worded highly technical scientific study.
We can only speculate the reason so many people have been reading it. But what this study suggests—which many clinicians and research scientists have expressed concerns about—is that COVID-19 mRNA vaccines as well as the booster shots may be making our immune response less effective against the Omicron variant of the virus.
If this is correct, it means that the vaccine itself is leading to widespread infection. Instead of stopping the virus, it appears that the mRNA vaccination programs around the world may have inadvertently made the virus more ubiquitous.
Analyzing why the most vaccinated populations are getting the most Omicron infections, this study focused on the most-vaccinated professionals: Medical personnel who had been given the two doses of mRNA vaccines early on, and were then given booster shots twice more. To find out what was happening on a cellular level with these highly vaccinated healthcare workers, the scientists kept close track of the different types of immunoglobin in the participants’ blood.
Immunoglobin (Ig), also known as antibody (Ab), finds viruses, bacteria, and such and leads the immune system to respond appropriately.
Scientists have identified several types of immunoglobulins, each guiding the immune response in a different way for different phases and types of infection.
IgG4 is the form of immunoglobin that activates a tolerance response in the immune system, for things you have been exposed to repeatedly and do not need to mount an inflammatory response to. This is good if you are trying to avoid immune sensitivity to a food, for example. But it is not the kind of immune response that the COVID-19 vaccines were designed to create.
Beekeepers, when they are repeatedly stung by bees over their career, mount an IgG4 response to the assault on their immune systems. Basically, their bodies learn that the bee venom is not dangerous and their immune response to bee venom becomes an IgG4 response, so they are able to tolerate the stings very well. While the bee venom itself will not harm the body, the body’s own inflammatory response can be dangerous.
If the body overreacts and develops a generalized response in which the inflammation itself jeopardizes a person’s breathing, the immune response can be lethal.
This study demonstrates exactly how the repeat vaccinations are causing people to be more susceptible to COVID-19. Initial doses of the vaccine brought about classic inflammatory immune responses. Inflammation is a fundamental part of an immune response (to a vaccine or to an infection), and is responsible for most of what you feel when you are sick: fever, aches, lethargy, etc. This inflammation is why you may feel sick if you get a flu shot, and why the COVID-19 vaccine has become famous for making people feel so sick for a few days. Your body is producing an inflammatory response to the COVID-19 proteins.
But what happens in the body after you have had two vaccines and then you are given a third? The scientists found that successive doses of the mRNA vaccines start to habituate or desensitize the subjects to the COVID-19 proteins, migrating their immune response over to being dominated by the IgG4 form, which essentially teaches the body to tolerate the proteins.

Don’t Fence Us In!
The participants’ response to COVID-19 had actually been turned off, making them even more vulnerable to infection and less likely to mount a response to it than those who had never been vaccinated.
When you are exposed to a cold or any other virus repeatedly, spaced out over a lifetime, which is what happens with natural exposure, you don’t develop a tolerance to it, your body fights it off without you knowing it. Your body is using the normal disease-fighting immune response but, since it recognizes the infectious agent, you do not get symptoms of inflammation. This is why when you are naturally exposed to many diseases, you then have lifelong immunity.
In contrast, this new study shows that the repeated mRNA injections and boosters for COVID-19 are producing a tolerance response, as if they were allergy shots. They are habituating the body to the virus, so that you no longer recognize it as something dangerous.
Another study, published in July by a team of more than 20 German scientists, independently confirmed that successive COVID-19 shots and boosters were converting the immune response from the protective class of IgG response to the toleration class.
Robert Malone writes at Brownstone Institute Delete the K in Monkeypox. Excerpts in italics with my bolds.
In a move that is sure to trigger widespread discussion concerning the independence, objectivity and wisdom of granting authority to the WHO to manage global infectious diseases responses, the monkeypox outbreak has been declared a Public Health Emergency of International Concern (PHEIC) by the World Health Organization.
The declaration was made unilaterally, in direct contradiction of independent review panel advice, by WHO director Tedros Adhanom Ghebreyesus. Tedros made the declaration despite a lack of consensus among members of the WHO’s emergency committee on the monkeypox outbreak, and in so doing overruled his own review panel, who had voted 9 against, 6 for declaring the PHEIC. Tedros asserted that this committee of experts (who met on Thursday) was unable to reach a consensus, so it fell on him to decide whether to trigger the highest alert possible.
When the group met in June, the breakdown was 11 against and three for. It is not clear what has changed in the intervening four weeks to justify the change in Tedros’ position, although comments from internet pundits raise concerns that the unilateral action was taken in response to pressure from special interest advocacy groups.
There has also been a sudden burst of coordinated social media postings raising concerns regarding Monkeypox risks to children, which raises the question “If Monkeypox is a sexually transmitted disease, why are kids getting it?”
On Friday, the U.S. confirmed the first two cases of monkeypox in children, Centers for Disease Control Prevention and Control (CDC) Director Rochelle Walensky said Friday. The CDC has said children, especially those under 8 years old, are among those at “especially increased risk” for severe monkeypox disease.
At a virtual event with the Washington Post on Friday focused on new coronavirus variants, Walensky stated that:
“Both of those children are traced back to individuals who come from the men-who-have-sex-with-men community, the gay men’s community,”
The WHO defines a PHEIC as “an extraordinary event which is determined to constitute a public health risk to other States through the international spread of disease and to potentially require a coordinated international response.”
The WHO further explains how this definition implies a situation that is serious, sudden, unusual or unexpected; carries implications for public health beyond an affected country’s border and may require immediate international action. Since the procedures to declare a PHEIC were implemented in 2005, the WHO has only done so six times. The last time was in early 2020, for Covid-19.
Tedros’ statements clearly demonstrate that he unilaterally substituted his own opinions for those of the convened panel, raising questions of his objectivity, commitment to process and protocol, and whether he has been unduly influenced by external agents.
As the outbreak continues to grow, epidemiologists are split as to whether the WHO’s decision was correct. The meeting was the second time the emergency committee convened, after a meeting on June 23 when it decided the outbreak had not met that threshold.
Dr. Jimmy Whitworth, a professor of international public health at the London School of Hygiene & Tropical Medicine:
“It is a tricky decision for the committee, in some senses, it meets the definition — it is an unprecedented outbreak widespread in many countries and would benefit from increased international coordination.
On the other hand, it seems to be an infection for which we have the necessary tools for control; most cases are mild and the mortality rate is extremely low.”
The PHEIC designation comes from the International Health Regulations (IHR) created in 2005, and it represents an international “agreement” to help the prevent and respond to public health risks that have the potential to spread around the globe.
These are the same IHR which the Biden administration sought to further strengthen, but the attempt to implement proposed modifications were placed on hold after an international, multi-country outcry concerning loss of national autonomy. The unilateral actions of Tedros in this current situation clearly demonstrate that these concerns were warranted.
In an article supportive of the declaration, Vox news provided a summary of the potential financial beneficiaries of this declaration; that being vaccine manufacturers and the holding companies who have invested in them.
The usual suspects are stirring the panic pot over Monkeypox, and so far our trusted sources of health guidance, like CDC and FDA and NIH, have been silent. So in the public interest I put forward a two-step program by which every individual can self-protect against Monkeypox.
1. Do not handle monkeys, squirrels or other rodents,
2. Do not have sex with anyone who does, or who has open skin sores.
There you go. Refrain from these two activities and no vaccine required.
More from Dr. Malone, who actually is trustworthy:
Don’t be Worried By Monkeypox (Unless it’s Genetically Altered!)
The usual suspects are stirring the panic pot over Monkeypox, and so far our trusted sources of health guidance, like CDC and FDA and NIH, have been silent. So in the public interest I put forward a two-step program by which every individual can self-protect against Monkeypox.
1. Do not handle monkeys, squirrels or other rodents,
2. Do not have sex with anyone who does, or who has open skin sores.
There you go. Refrain from these two activities and no vaccine required.
More from Dr. Malone, who actually is trustworthy:
Don’t be Worried By Monkeypox (Unless it’s Genetically Altered!)

As we approach autumn in the NH, already the medical-governmental complex is gearing up for another takeover of individual rights and freedoms. New medications (pale, dangerous ivermectin imitations) and more experimental shots have been approved in readiness for imminent mandates requiring their use, This is a time to remember, not forget, how a fake pandemic was foisted upon the world. Yes, runny nose coronaviruses are real and have been in circulation worldwide for decades. But the threat was never great for the large majority of populations, and anti-viral treatments were available despite intimidation against them. Like the four horsemen of the apocalypse, four myths are saddling up again to ride over our peace and harmony.
Jack Kerwick has written a series of articles at FrontPage Mag over the last year discussing how facts have been overwhelmed by fears, a mythology replacing scientific knowledge and reason. From the beginning this contagion was different, being the first one in an age of 24/7 cable news and rampant social media. So emotion and exaggeration were spread and political leaders pressured to act as protectors, clamping down on social and economic transactions. This post provides a synopsis of what went wrong, based on Kerwick’s recent essay Masks and Stopping COVID. Excerpts in italics with my bolds.
What the science – lots of science – really tells us.
In previous essays, I argued for three theses against the prevailing COVID Orthodoxy:
Has the existence of “the Virus” been established according to a universally acknowledged set of scientific procedures that must be observed to establish the existence of any and all other viruses?
From the sounds of it, the answer is a resounding no.
Dr. Tom Cowan, Dr. Andrew Kaufman, and Sally Fallon Morell, are among those who have noted in a paper published last year that in demonstrating the existence of a new virus, samples must, firstly, be taken from the blood, phlegm, or other secretions of hundreds of people exhibiting symptoms that are “unique and specific enough to characterize an illness.”
Then, “without mixing these samples with ANY tissue or products that also contain genetic material, the virologist macerates, filters, and ultracentrifuges, i.e. purifies the specimen.” This, the authors explain, is a “common virology technique, done for decades to isolate bacteriophages [viruses that infect bacteria and reproduce within them] and so-called giant viruses [a virus larger than typical bacteria].”
Thirdly, once virologists perform this procedure, they are then able to “demonstrate with electron microscopy thousands of identically sized and shaped particles.” The latter are “the isolated and purified virus.”
Fourthly, upon determining the purity of these particles, virologists are able to examine their “structure, morphology, and chemical composition [.]”
Fifthly, “the genetic makeup” of the particles [the virus] “is characterized by extracting the genetic material directly from” them and “using genetic-sequencing techniques” that have long been in existence.
Finally, an analysis must be conducted to prove that “these uniform particles are exogenous (outside) in origin” as viruses are held to be and not just “the normal breakdown of products of dead and dying tissues.”
The authors conclude: “If we have come this far then we have fully isolated, characterized, genetically-sequenced an exogenous virus particle” .
They add that nowhere in the literature does it show that any of these steps have been taken with respect to SARS-CoV-2.
Neither—and this is crucial—have the scientific steps for determining that SARS-CoV-2 is the cause of a disease, COVID-19, been taken. What are these steps? There really isn’t much to it:
A group of healthy subjects, typically animals, is first exposed to “this isolated, purified virus in the manner in which the disease is thought to be transmitted.”
Subsequently, virologists will wait to determine whether these subjects fall ill with “the same disease, as confirmed by clinical and autopsy findings [.]” If so, “one has now shown that the virus actually causes a disease.” In other words, the “infectivity and transmission of an infectious agent” will have been demonstrated.
Again, according to the authors, nothing like this has been performed to show that
there is a virus, SARS-CoV-2, that causes what has become known as COVID-19.
An ever growing number of citizen journalists in over ten different countries from around the world have, via the Freedom of Information Acts of their respective homes, requested from scores of health agencies an account of the process by which SARS-CoV-2 has been isolated (i.e. separated out from all other stuff). To date, no account has been provided.
The official case numbers, in other words, are meaningless.
Right from the jump, it’s crucial to take note of the fact that for the first time ever, beginning just last year, “cases” was radically redefined in such a way that would have been unthinkable in just February of 2020 (one month before The Virus Apocalypse engulfed the universe).
For starters, as indicated above, many of these “cases,” per the CDC, included those patients who were labeled as “probable” carriers of the virus. This means that they were diagnosed as “cases” in the absence of any “confirmatory laboratory testing.” And yet they were identified as COVID “cases.”
Moreover, even when testing is figured into it, with respect to no other virus or disease has the CDC ever counted as a “case” a merely positive test. A positive test, in other words, has never been regarded by the medical establishment as sufficient grounds upon which to determine a “case.” Rather, in order for something to count as a “case,” a person had to have been sick and in need of medical attention like, say, hospitalization.
In the COVID era, however, the CDC began accumulating positive PCR test results (about more of which will be said below) from people the vast majority of whom are “asymptomatic,” meaning they feel just fine, and combining them with positive antibodies tests from people who also feel just fine: The final sum, this compound, comprises all “cases.”
Now, as for those PCR tests: There are two problems.
First, as Karry Mullis bluntly remarked: “Quantitative PCR is an oxymoron.” Who was Karry Mullis? He was the inventor of the PCR test. And he won a Nobel Prize in Science for this achievement. What did the late Dr. Mullis mean by his characterization of his own invention?
“PCR is intended to identify substances qualitatively, but by its very nature is unsuited for estimating numbers [of viruses]. Although there is a common misimpression that the viral load tests actually count the number of viruses in the blood, these tests cannot detect free, infectious viruses at all; they can only detect proteins that are believed, in some cases wrongly, to be unique to HIV. The tests can detect genetic sequences of viruses, but not viruses themselves” (emphases added).
Lauitsen explains further:
“What PCR does is to select a genetic sequence and then amplify it enormously. It can accomplish the equivalent of finding a needle in a haystack; it can amplify that needle into a haystack. Like an electronically amplified antenna, PCR greatly amplified the signal, but it also greatly amplifies the noise” (emphases added).
What this implies is that given that “the amplification is exponential, the slightest error in measurement, the slightest contamination, can result in errors of many orders of magnitude.”
There is still another problem with the PCR test as it is currently being used that guarantees its utter worthlessness. More exactly, that guarantees that the “case” numbers built upon it are wholly inaccurate and, hence, meaningless.
This past fall, none other than the New York Times noted that possibly as high as 90% of all positive test results are false.
Per the CDC and FDA guidelines, the vast majority of PCR tests are run at a threshold of 40 cycles. Dr. Michael Mina, an epidemiologist from Harvard who is quoted in the Times piece, notes that when PCR tests are run at 35 or more cycles, they “may detect not just live virus but also live fragments, leftovers from infection that pose no particular risks—akin to finding a hair in a room long after a person has left.”
The French researcher Didier Raoult has shown that when the PCR test is run at 25 cycles, about 70% of samples were genuinely positive—meaning infectious. However, when the test is run at a threshold of 30 cycles, only 20% of samples were infectious. At 35 cycles, but three percent of samples were infectious.
And when the test was run above 35 cycles? Zero samples were infectious.
Think about it: a cough, running nose, sore throat, chills, chest congestion, fever, loss of taste and smell—these are all symptoms of a plethora of things, from the common cold to seasonal influenza and a whole lot else. Particularly since the vast majority of COVID cases are “mild,” it’s with the greatest of ease that any single one of these symptoms or any number of combinations of them can be used as a pretext by which to establish a “COVID case.”
This is not necessarily to say that the symptoms in question are not signs of COVID or the SARS-CoV-2 virus that is claimed to be its cause. It’s only to note that in the absence of scientifically confirming definitively that (a) there is a unique strain of a coronavirus called SARS-CoV-2, (b) that it is the cause of something called COVID-19, and that, (3) given the scandalously unreliable PCR test, people do in fact have COVID, symptoms that are associated with the latter are more economically, more plausibly explained by way of reference to illnesses that have long been with us.
The Principle of Parsimony—better known since the 14th century as “Ockham’s Razor”—applies: When confronted with two or more explanatory hypotheses, all things being equal, reason dictates that we opt for the one that is simplest.
Since many of the symptoms now being associated with COVID until recently were explained in terms of, say, the flu, and, given the foregoing facts regarding the science—or lack of science—behind the COVID Narrative, it makes better sense to continue explaining those symptoms in terms of the flu.
Indeed, there is no doubt that a great shell game has been transpiring for a year now as cases of various illnesses have been re-labeled as COVID cases.
For example, over at John Hopkins University, Genevieve Briand, assistant program director of the Applied Economics master’s program, used data from the CDC to analyze the effect of COVID-19 deaths in America on all other deaths. Reasonably enough, she had expected to witness a substantial number of excess deaths in 2020, i.e. deaths by all other causes plus the orgy of COVID deaths with which politicians and those in the media had been singularly preoccupied.
She was mistaken. Sorely mistaken. Yanni Gu, a writer for the university’s student newspaper, reports: “Surprisingly, the deaths of older people stayed the same before and after COVID-19.”
This was surprising because COVID (not unlike virtually everything else) overwhelmingly affects elderly people. Thus, “experts expected an increase in the percentage of deaths in older age groups. However, this increase is not seen from the CDC data.” Furthermore, “the percentages of deaths among all age groups remain relatively the same” (emphases added).
Whoa. Briand would soon discover that the plot was just beginning to thicken. What the “data analyzes suggest,” Gu writes, is “that in contrast to most people’s assumptions, the number of deaths by COVID-19 is not alarming. In fact, it has relatively no effect on deaths in the United States” (emphases added).
There is a perfectly rational, and simple, explanation to account for the unbridgeable chasm between the media-concocted perception of COVID and the reality that Briand discovered:
Deaths from all other causes were being re-classified—misclassified—as death from COVID. And how did Briand determine this?
For the first time ever, deaths from all other causes—heart diseases, respiratory diseases, influenza, and pneumonia—decreased.
Especially shocking was the realization that heart disease, which has always been the number one killer in America, appeared to have suddenly lost that distinction with the onset of COVID.
Moreover, deaths from all other causes decreased just in proportion to the extent to which COVID deaths increased. “This trend is completely contrary to the pattern observed in all previous years. Interestingly…the total decrease in deaths by other causes almost exactly equals the increase in deaths by COVID-19.”
Within 24 or so hours of the publication of the article relaying Genevieve Briand’s discoveries, the student paper at John Hopkins University retracted it. They never, however, denied the truth of a single syllable of either Briand’s analysis nor its summary of it. That it was political pressure, and not shoddy scholarship that informed its decision is clear, for the school paper saved its article in a PDF file (to which I link above) for all of the world to read.
In this essay, we will revisit the topic of masks. I’ve already written about the psychological, moral, and social costs of mask-wearing. Here, I will focus specifically on the science—or lack of science—behind it.
Scientists recognize that the RCT—Randomized Control Trial—is the “gold standard” as far as “effectiveness research” is concerned. Drs. Eduardo Hariton and Joseph J. Locasio explain that randomization “reduces bias” while providing “a rigorous tool” by which “to examine cause-effect relationships between an intervention and outcome.” RCTs eliminate the risk of confirmation bias, something that is “not possible with any other study design” (emphases added).
This is critical for our purposes, for the largest study of the effectiveness of mask-wearing by the general public to thwart the transmission of COVID utilized not one, not two, not three, but a staggering 14 randomized control trials.
The study was performed at the University of Hong Kong. What Dr. Jingyi Xiao and her team of researchers there concluded will doubtless be written off as the stuff of “conspiracy theorists” by Mask Nation. So be it. But those on the editorial board of Emerging Infectious Diseases, the widely esteemed journal of none other than the Centers for Disease Control and Prevention (CDC), determined that the findings were worth publishing.
The verdict: Masks are ineffective.
The authors of a review of studies on face masks published last year by the Oxford Centre for Evidence-Based Medicine determined that there is no evidence indicating the effectiveness of cloth masks when it comes to COVID. They lament how the “abandonment of the scientific modus operandi and lack of foresight has left the field [of science] wide open for the play of opinions, radical views and political influence.”
The authors, one an epidemiologist, the other a professor of Evidence-Based Medicine at Oxford, do note that all randomized control trials that have been conducted over the last decade or so have demonstrated that “masks alone have no significant effect in interrupting the spread of ILI [Influenza-Like-Illness] or influenza” in neither “the general population…nor in healthcare workers” (emphases added).
We could continue in this same repetitive vein. Readers who are interested in pursuing this topic further can check out this piece of mine from October of last year. I review still other studies there, including remarks from such media-adored “Experts” as Anthony Fauci that dovetail seamlessly with these findings on the essential uselessness of masks with respect to COVID. More research confirming these findings are here, here, here, here, and here. Neither have we yet touched upon the numerous studies showing that countries and states with mask mandates did no better and, in some instances, worse than those places that had no such mandates. Nor have we looked at those studies demonstrating that those who faithfully wore masks were not less likely to contract COVID than those who did not wear masks, with some of these—like this one from the CDC—showing that most people who became infected with COVID wore a mask “always” or “often.”
The science, it should now be obvious, does not support Mask dogma.

Marty Makary and Tracy Beth Høeg write at commonsense.news U.S. Public Health Agencies Aren’t ‘Following the Science,’ Officials Say. It’s another stark example how politicizing institutions by requiring fidelity to the party line leads to paralysis and dysfunction. Excerpts in italics with my bolds and added images.
‘People are getting bad advice and we can’t say anything.’

The calls and text messages are relentless. On the other end are doctors and scientists at the top levels of the NIH, FDA and CDC. They are variously frustrated, exasperated and alarmed about the direction of the agencies to which they have devoted their careers.
“It’s like a horror movie I’m being forced to watch and I can’t close my eyes,” one senior FDA official lamented. “People are getting bad advice and we can’t say anything.”
That particular FDA doctor was referring to two recent developments inside the agency. First, how, with no solid clinical data, the agency authorized Covid vaccines for infants and toddlers, including those who already had Covid. And second, the fact that just months before, the FDA bypassed their external experts to authorize booster shots for young children.
That doctor is hardly alone.
At the NIH, doctors and scientists complain to us about low morale and lower staffing: The NIH’s Vaccine Research Center has had many of its senior scientists leave over the last year, including the director, deputy director and chief medical officer. “They have no leadership right now. Suddenly there’s an enormous number of jobs opening up at the highest level positions,” one NIH scientist told us. (The people who spoke to us would only agree to be quoted anonymously, citing fear of professional repercussions.)
The CDC has experienced a similar exodus. “There’s been a large amount of turnover. Morale is low,” one high level official at the CDC told us. “Things have become so political, so what are we there for?” Another CDC scientist told us: “I used to be proud to tell people I work at the CDC. Now I’m embarrassed.”
Why are they embarrassed? In short, bad science.
The longer answer: that the heads of their agencies are using weak or flawed data to make critically important public health decisions. That such decisions are being driven by what’s politically palatable to people in Washington or to the Biden administration. And that they have a myopic focus on one virus instead of overall health.
Nowhere has this problem been clearer—or the stakes higher—than on official public health policy regarding children and Covid.
First, they demanded that young children be masked in schools. On this score, the agencies were wrong. Compelling studies later found schools that masked children had no different rates of transmission. And for social and linguistic development, children need to see the faces of others.
Next came school closures. The agencies were wrong—and catastrophically so. Poor and minority children suffered learning loss with an 11-point drop in math scores alone and a 20% drop in math pass rates. There are dozens of statistics of this kind.
Then they ignored natural immunity. Wrong again. The vast majority of children have already had Covid, but this has made no difference in the blanket mandates for childhood vaccines. And now, by mandating vaccines and boosters for young healthy people, with no strong supporting data, these agencies are only further eroding public trust.
One CDC scientist told us about her shame and frustration about what happened to American children during the pandemic: “CDC failed to balance the risks of Covid with other risks that come from closing schools,” she said. “Learning loss, mental health exacerbations were obvious early on and those worsened as the guidance insisted on keeping schools virtual. CDC guidance worsened racial equity for generations to come. It failed this generation of children.”
An official at the FDA put it this way: “I can’t tell you how many people at the FDA have told me, ‘I don’t like any of this, but I just need to make it to my retirement.’”

Three weeks ago, the CDC vigorously recommended mRNA Covid vaccines for 20 million children under five years of age. Dr. Rochelle Walensky, director of the CDC, declared that the mRNA Covid vaccines should be given to everyone six months or older because they are safe and effective.
The trouble is that this sweeping recommendation was based on extremely weak,
inconclusive data provided by Pfizer and Moderna.
Start with Pfizer. Using a three-dose vaccine in 992 children between the ages of six months and five years, Pfizer found no statistically significant evidence of vaccine efficacy. In the subgroup of children aged six months to two years, the trial found that the vaccine could result in a 99% lower chance of infection—but that they also could have a 370% increased chance of being infected. In other words, Pfizer reported a range of vaccine efficacy so wide that no conclusion could be inferred. No reputable medical journal would accept such sloppy and incomplete results with such a small sample size. More to the point, these results should have given pause to those who are in charge of public health.
Referring to Pfizer’s vaccine efficacy in healthy young children, one high-level CDC official—whose expertise is in the evaluation of clinical data—joked: “You can inject them with it or squirt it in their face, and you’ll get the same benefit.”
Moderna’s results—they conducted a study on 6,388 children with two doses—were not much better. Against asymptomatic infections, they claimed a very weak vaccine efficacy of just 4% in children aged six months to two years. They also claimed an efficacy of 23% in children between two and six years old—but neither result was statistically significant. Against symptomatic infections, Moderna’s vaccine did show efficacy that was statistically significant, but the efficacy was low: 50% in children aged six months to two years, and 42% in children between two and six years old.
Then there’s the matter of how long a vaccine gives protection. We know from data in adults that it’s generally a matter of months. But we have no such data for young children.
“It seems criminal that we put out the recommendation to give mRNA Covid vaccines to babies without good data. We really don’t know what the risks are yet. So why push it so hard?” a CDC physician added. A high-level FDA official felt the same way: “The public has no idea how bad this data really is. It would not pass muster for any other authorization.”
This isn’t the first time that Covid vaccines recommendations based on scant evidence have been pushed through these agencies.
Most recently, back in May, the lack of clinical evidence for booster shots in young people created a stir at the FDA. The White House promoted it hard even before FDA regulators had seen any data. Once they saw the data, they weren’t impressed. It showed no clear benefit against severe disease for people under 40.
The FDA’s two top vaccine regulators—Dr. Marion Gruber, director of the FDA’s vaccine office, and her deputy director, Dr. Philip Krause—quit the agency last year over political pressure to authorize vaccine boosters in young people. After their departure they wrote scathing commentaries explaining why the data did not support a broad booster authorization, arguing in the Washington Post that “the push for boosters for everyone could actually prolong the pandemic,” citing concerns that boosting based on an outdated variant could be counterproductive.
“It felt like we were a political tool” a CDC scientist told us about the issue. That insider went on to explain that he got vaccinated early but chose not to get boosted based on the data. Ironically, that person was unable to go on a trip with a group of parents because proof of being boosted was required. “I asked for someone to show me the data. They said the policy was based on the CDC recommendation.”
As one NIH scientist told us: “There’s a silence, an unwillingness for agency scientists to say anything. Even though they know that some of what’s being said out of the agency is absurd.”
That was a theme we heard over and over again—people felt like they couldn’t speak freely, even internally within their agencies. “You get labeled based on what you say. If you talk about it you will suffer, I’m convinced,” an FDA staffer told us. Another person at that agency added: “If you speak honestly, you get treated differently.”
It is statistically impossible for everyone who works inside of our health agencies to have 100% agreement about such a new and knotty subject. The fact that there is no public dissent or debate can only be explained by the fact that they are—or at least feel that they are—being muzzled.
It is an ancient, moral requirement of our profession to speak up when we believe questionable treatments are being proposed. It is also good for the public. Imagine, for example, a world in which those scientists who suggested that masking for children and school lockdowns were worse for public health were not smeared but instead debated?
The official public health response to Covid has undermined
the public’s belief in public health itself.
This is a terrible outcome with potentially disastrous consequences. For one thing, because of these sloppy and politicized policies, we run the risk of parents rejecting routine vaccines for their children—ones we know are safe, effective and life-saving.
The leaders of the CDC, the FDA and the NIH should welcome internal discussion—even dissension—based on the evidence. Silencing physicians is not “following the science.” Less absolutism and more humility by the men and women running our public health agencies would go a long way in rebuilding public trust.

Yesterday waiting for pharmacists to fill my wife’s prescription, I noticed the info tv on the wall displayed something like the above. I knew this government spent two years insisting only vaccines had any effect on covid19, and disavowed any and all treatments of people sick from covid19, including HCQ and Ivermectin. Naturally, I was curious to know what treatment they now approved for public consumption.
Would you believe it? They are offering Paxlovid to people to alleviate their suffering after testing positive for Covid19. Is there any public service more totally captured by suppliers than the Public Health Establishment?

On Tuesday, Dr. Anthony Fauci confirmed that he is experiencing “COVID rebound” after taking Pfizer’s Paxlovid, the so-called silver bullet that Biden wasted billions in taxpayer dollars to support.
Paxlovid appears to have almost zero effectiveness for people that are already vaccinated, according to the manufacturer Pfizer’s data.
Fauci, shared his health update while speaking remotely at the Foreign Policy Global Health Forum.
Earlier in June, Fauci tested positive for the virus with mild symptoms, including fatigue. According to Fauci, as his symptoms worsened, he began a five-day course of the supposed wonder drug.
When talking about his experience with the medication, Fauci said that he tested negative for the virus three days in a row. However, when he tested again on the fourth day, the test was positive again.
Fauci said that his symptoms were “much worse” after he tested positive for the second time following the treatment with Paxlovid.
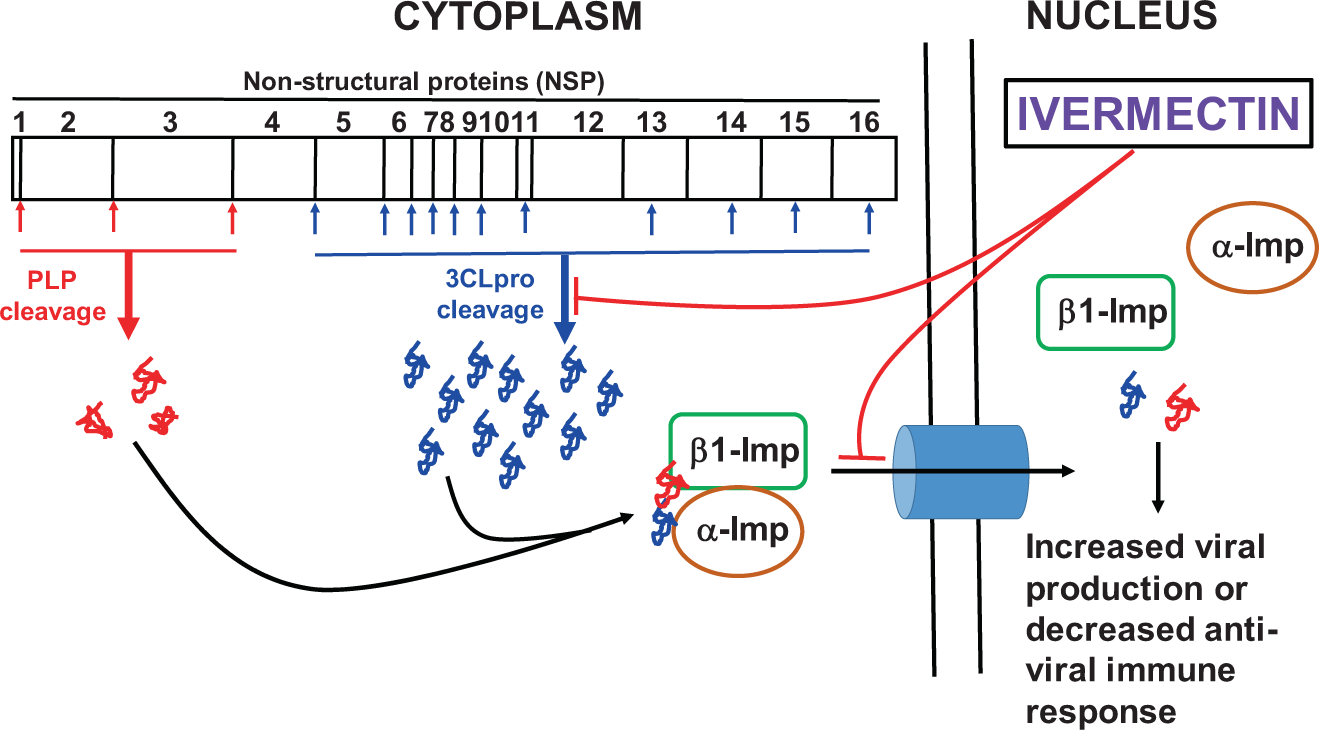
Hypothetical model illustrating the inhibition of SARS-CoV-2 replication by ivermectin mediated through the blocking of α/β1-importin (imp) as well as 3CLpro enzymatic activity. Mody et al (2021)
The Medical Pharmaceutical Industrial complex waged psy-ops warfare against effective and safe generic medicines, including hydroxychloroquine and ivermectin. Now FDA approves pills from Pfizer and Merck for “emergency use”, and in Quebec where I live, they follow along like lemmings rolling out Paxlovid, claiming the pill is a “game changer.” All this ignores that once again trials have been compressed so that longer term side effects are unknown, and Pfizer and Merck have no liability while expecting billions in profits.
As the background post below shows in some detail, these pills are not only pale substitutes for the proven generic therapeutics, they risk stimulating further viral mutations and prolonging the infectious activity in vaccinated and pill-popping developed societies. Fortunately, Africa and much of Asia and South America will be spared this latest public health experiment, as they have natural covid immunity from the virus itself with HCQ and IVM protecting people from severe illnesses.

John Campbell explains in the video below how the new Pfizer pill copies one trick from Ivermectin, without IVM’s other anti-viral mechanisms, resulting in an inferior and dangerous medicine. I have transcribed the basic message along with excerpts and links to several papers to which he refers. Excerpts are in italics with my bolds.
Pfizer’s new antiviral drug PAXLOVID™ shows very high levels of efficacy in preventing serious disease hospitalization and people dying. And that drug works in a particular way, what we call a pharmacodynamic action.
But there’s another generic drug called Ivermectin that you might have heard of that works in exactly the same way as that. Now no one’s saying that information has been deliberately suppressed for years while millions of people have died but what we are going to show on this video is conclusive proof from the literature that this modality of action is the same.
Before we crack into that we need to look at what’s happening so when a virus, in this case coronavirus2 gets into a cell. What happens is it makes lots of proteins. It starts off making these long proteins, out of hundreds of amino acids sometimes. A few thousand amino acids all strung together.
The problem is they’re too long for the job that’s required. So it’s a bit like a building site and when a big log of wood arrives it needs to be trimmed down into bits that fit in your door frames and your window frames. So these proteins need to be trimmed down and it has to be done in a biochemical way.
In the case of coronavirus two, there’s an enzyme called 3CL protease which breaks
down protein into smaller pieces. it’s what we call proteolytic and it will take these long proteins and it will chop them into shorter proteins it’s what we call an endopeptidase. So now instead of having one long protein we’ve got two short ones and these fit together just nicely for the new virus that we’re we’re trying to make.
These new drugs are what we call protease inhibitors because they stop the protease from working. If the protease is like this scissor, the inhibitor is like this tape stopping the cutting up of long proteins.
When there’s another long protein that needs to be processed the 3CL protease comes along ready to chop this up. But now these drugs have bounded up the active site of the protease and they stop the protease from chopping up the big proteins into smaller strings of amino acids. Since they can’t build the virus, it inhibits viral replication.
This is the new Pfizer drug which is designed to block the activity of the sars coronavirus2 3CL, so that 3CL protease now won’t work. It won’t open so i can’t chop my proteins into the correct length to build a nice new virus. And of course a 3CL protease inhibitor will stop it from making sars coronavirus2 and is therefore anti-viral.
Everyone in human biology has heard of chymotryptin. It’s an enzyme released by the pancreas to digest protein. It’s a protein chopping up enzyme so this chymotryptin-like protease inside the virus is working in a very similar way to the chimbotryptin that your pancreas produces to digest your proteins.
Evidence from Pfizer News Release
If approved or authorized, PAXLOVID™, which originated in Pfizer’s laboratories, would be the first oral antiviral of its kind, a specifically designed SARS-CoV-2-3CL protease inhibitor. Upon successful completion of the remainder of the EPIC clinical development program and subject to approval or authorization, it could be prescribed more broadly as an at-home treatment to help reduce illness severity, hospitalizations, and deaths, as well as reduce the probability of infection following exposure, among adults. It has demonstrated potent antiviral in vitro activity against circulating variants of concern, as well as other known coronaviruses, suggesting its potential as a therapeutic for multiple types of coronavirus infections.
Identification of SARS-CoV-2 3CL Protease Inhibitors by a Quantitative High-Throughput Screening Zhu et al. (Sept 3, 2020)
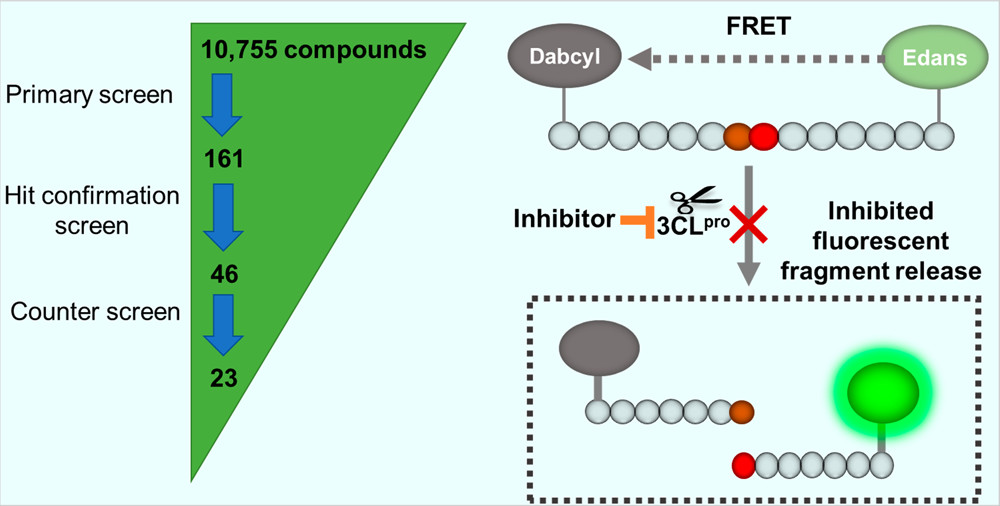
Viral protease is a valid antiviral drug target for RNA viruses including coronaviruses. (13) In response to the COVID-19 pandemic, great efforts have been made to evaluate the possibility of repurposing approved viral protease inhibitor drugs for the clinical treatment of the disease. Unfortunately, the combination of lopinavir and ritonavir, both approved HIV protease inhibitors, failed in a clinical trial without showing benefit compared to the standard of care. (14) To address this unmet need, several virtual screens and a drug repurposing screen were performed to identify SARS-CoV-2 3CLpro inhibitors.
In conclusion, this study employed an enzymatic assay for qHTS that identified 23 SARS-CoV-2 3CLpro inhibitors from a collection of approved drugs, drug candidates, and bioactive compounds. These 3CLpro inhibitors can be combined with drugs of different targets to evaluate their potential in drug cocktails for the treatment of COVID-19. In addition, they can also serve as starting points for medicinal chemistry optimization to improve potency and drug-like properties.
Identification of 3-chymotrypsin like protease (3CLPro) inhibitors as potential anti-SARS-CoV-2 agents Mody et al. (2021), source of diagram at top. Excerpts in italics with my bolds.
Fig. 4: Ivermectin exhibited complete inhibition of SARS-CoV-2 3CLpro enzymatic activity whereas micafungin partially inhibited the enzyme.
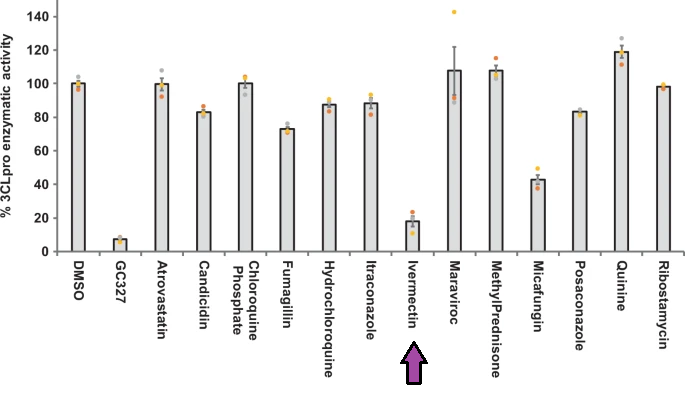
The off-target drugs that are being used to treat non-viral ailments selected by in silico studies were screened for their inhibitory activity against SARS-CoV-2 3CLpro enzyme.
Interestingly, one of the OTD (Off Target Drugs), ivermectin was able to inhibit more than 85% (almost completely) of 3CLpro activity in our in vitro enzymatic assay with an IC50 value of 21 µM. These findings suggest the potential of ivermectin to inhibit the SARS-CoV-2 replication. In support of this, a recent finding suggested that ivermectin (5 µM) inhibited the replication of live SARS-CoV-2 isolated from Australia (VIo1/2020) in Vero/hSLAM cells23. They found that >5000-fold viral counts were reduced in 48 hr in both culture supernatant (release of new virion: 93%) as well as inside the cells (unreleased and unassembled virion: 99.8%) when compared to DMSO treated infected cells.
Earlier studies have demonstrated that the possible anti-viral mechanism of ivermectin was through the blockage of viral-protein transportation to the nucleus by inhibiting the interaction between viral protein and α/β1 importin heterodimer, a known transporter of viral proteins to the nucleus especially for RNA viruses19,20,21,22,23. However, in this study, we have reported that ivermectin inhibits the enzymatic activity of SARS-CoV-2 3CLpro and thus may potentially inhibit the replication of RNA viruses including SARS-CoV-2. These studies suggest that ivermectin could be a potential drug candidate to inhibit the SARS-CoV-2 replication and the proposed anti-viral mechanism of ivermectin presented in Fig. 8 and in vivo efficacy of ivermectin towards COVID-19 is currently been evaluated in clinical trials (ClinicalTrials.gov Identifier: NCT04438850).
Inhibitor of SARS-CoV-2 key target proteins in comparison with suggested COVID-19 drugs: designing, docking and molecular dynamics simulation study. Excerpts in italics with my bolds.
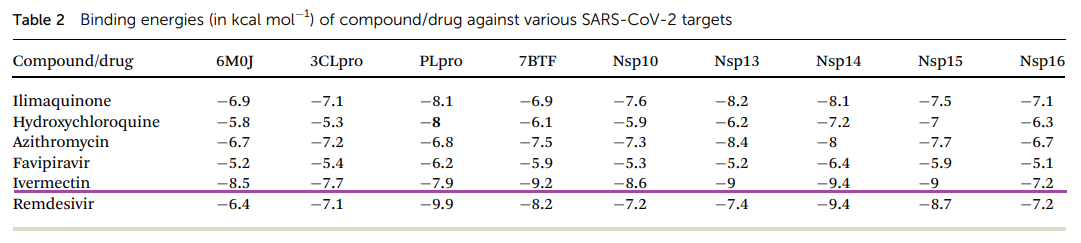
Double-click on image to enlarge.
In conclusion, both ivermectin and remdesivir could be considered potential drugs for the treatment of COVID-19. Ivermectin efficiently binds to the viral S protein as well as the human cell surface receptors ACE-2 and TMPRSS2; therefore, it might be involved in inhibiting the entry of the virus into the host cell. It also binds to Mpro and PLpro of SARS-CoV-2; therefore, it might play a role in preventing the post-translational processing of viral polyproteins. The highly efficient binding of ivermectin to the viral N phosphoprotein and nsp14 is suggestive of its role in inhibiting viral replication and assembly. Remdesivir may be involved in inhibiting post-entry mechanisms as it shows high binding affinity to N and M proteins, PLpro, Mpro, RdRp, and nsp14. Although the results of clinical trials for remdesivir are promising (Beigel et al., 2020; Wang Y. et al., 2020), similar clinical trials for ivermectin are recommended. Both these drugs exhibit multidisciplinary inhibitory effects at both viral entry and post-entry stages. Source: Molecular Docking Reveals Ivermectin and Remdesivir as Potential Repurposed Drugs Against SARS-CoV-2
So whereas the Pfizer drug is only working as far as we’ve been told in the proviso press release against one biochemical modality of viral replication, the Ivermectin mechanism is working at many different levels. The fact that the the the Pfizer medicine is only working against one particular biochemical pathway means to me that the virus could learn to avoid that. It could evolve to be drug resistant as indeed the early antiretrovirals did with HIV.
With ivermectin, because it’s working on so many different levels, it is improbable, to put it mildly,that a virus would mutate in a dozen different ways to avoid all those different mechanisms. We’ve talked about six mechanisms today. It’s very unlikely that we get six mutations that could dodge all of those all at the same time.
So I’ve a brief message to world leaders, people that are making the decisions about this. Come on you all, you’re not a horse and you’re not a cow. You’ve got a human intellect. Let’s use it to follow the scientific evidence to save human pain, suffering and death.
Comment
Ivermectin is the most successful and proven protease inhibitor in production. Just as with Paxlovid, ivermectin decreases the protease enzyme but…the benefits of ivermectin in Covid treatment are obvious and not present in paxlovid. Additional actions of ivermectin include anti-coagulant action and anti-inflammatory actions, both observed in Covid infections. Hydroxychloroquine is also a protease inhibitor and also works against COVID.
So why PAXLOVID? Because it’s from big pharma, is less proven than other drugs in terms of safety, and was approved without input from the external committees and the public. If that inspires confidence, then I don’t know what will give you pause.
Footnote: This video focused on Pfizer’s pill, but Merck’s Molnupiravir pill is also a one-trick-pony. See Why Merck Dissed Its Own Invention Ivermectin