Clueless Covid Policies

In recent months, some demonstrators in Quebec have denounced what they consider government fear campaigns over COVID-19. The new measures included a mandatory rule on wearing masks during demonstrations. (Graham Hughes/The Canadian Press)
A previous post discussed how policymakers are imposing draconian restrictions on their citizens in a misguided attempt to stop viral infections. The basic fallacy is this:
It seems that certain disease experts genuinely believe that they can game the reproduction rate of the virus to get it below 1, and thereby create a mathematical result that will make the virus go away.
This seems to be their goal and the metric by which they measure whether and to what extent they have achieved it. The problem is that the reproduction rate (very difficult to discern precisely) is an effect – a measurement of an evolved condition – not a cause.
Previous Post Covid Coercion in Quebec
Update: Quebec is one example of a world wide problem: See COVID-19 Is Also a Crisis for Democracy and Human Rights
The coronavirus pandemic began as a global health crisis. It spawned an economic crisis. Now COVID-19 is also fueling a crisis for democracy and human rights.
Leaders around the world are using the virus as cover to reduce transparency, increase surveillance, arrest dissidents, repress marginalized populations, embezzle public resources, restrict media, and undermine fair elections.

What is the Emergency Requiring Virtual Quarantine of Healthy People?
![]()
Each Friday the Quebec health research institute (INESSS) provides a statistical update of the Covid19 situation with projections regarding the key concern: Capacity of the system to care for actual Covid cases requiring in-hospital treatment. Here is the latest information from October 28, 2020.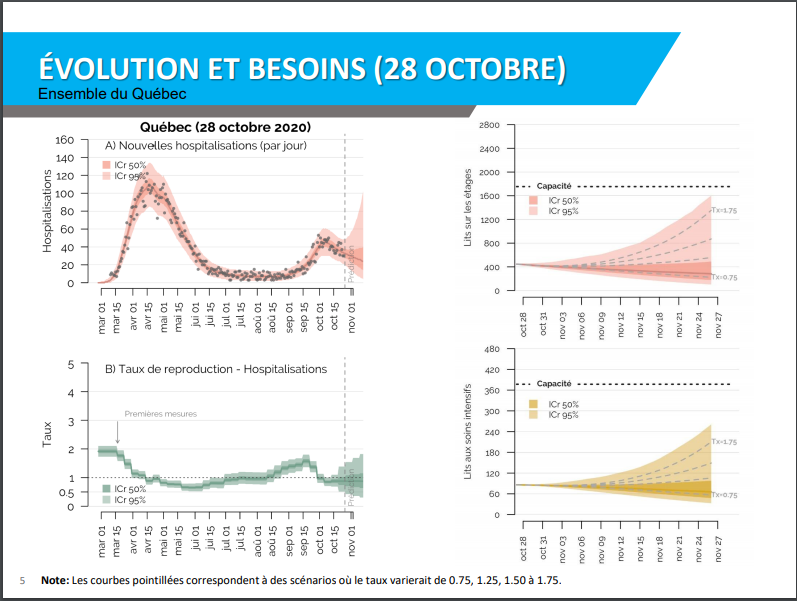
On the left is the history of Covid hospitalizations in Quebec to end of September. Note admissions peaked in April around 120 per day, then dropped to 20 a day June to September. A “second wave” was feared but the graph shows only a bump up to 50 mid October falling already. As of Oct. 28, Quebec reported 439 people in hospital out of covid bed capacity of 1750. In addition 88 were in ICUs out of a capacity of 380. At a 30/day new admissions rate, and assuming an average length of stay of 12 days, the net of covid beds occupied should not increase and more likely would go down. So the projections on the right side have a wide range, but show declining numbers of Covid patients in hospital. And as the lower right shows, demand for ICU capacity is is also expected to diminish.
On September 24, INESSS authorities said (here):
In Quebec, the hospitalization rate for COVID-19 patients has dropped sharply since the beginning of the pandemic. During the first wave, about 13 per cent of cases ended up in hospital. From Aug. 10 to Sept. 6, the rate was just 5 per cent. At a technical briefing on Wednesday, researchers and officials from Quebec’s institute of excellence in health and social services (INESSS) projected that the rate for COVID-19 patients in early September would fall again to 3.8 per cent.
The drop can be explained by the relative youth of Quebeckers contracting the virus in its second wave and their relative lack of comorbidities. By contrast, in the spring, the virus tore through long-term care homes in the province, killing 4,914 elderly residents.
As a result of this shift, Quebec will not exceed its hospital capacity of about 2,000 beds in the next four weeks, according to the INESSS projections. But officials warned that a faster spread of the virus caused by careless behaviour could still put pressure on the health care system.
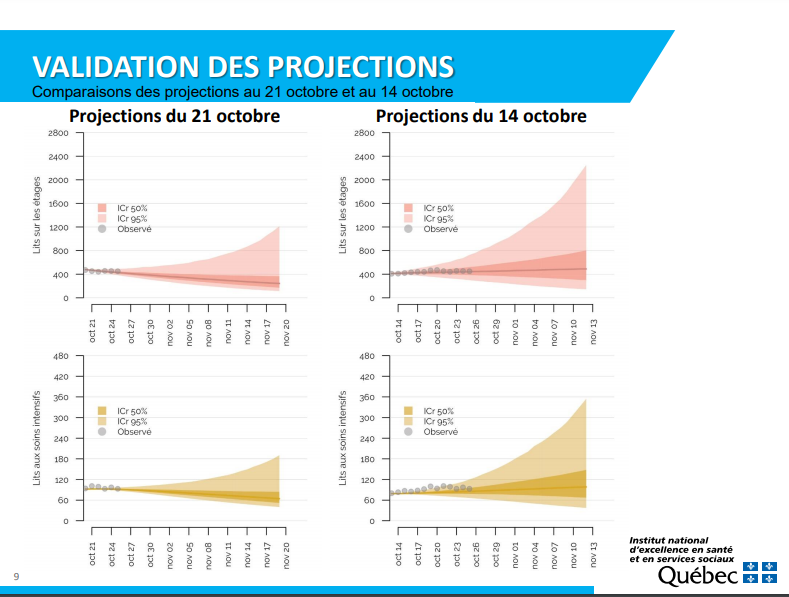
Above is the outlook for October from INESSS. For both ICU and covid hospital beds observations are tracking a forecast showing slight increases. It appears that the precautionary principle is being applied without regard for the costs of locking down: social, economic and personal well-being seem not to be part of the equation.
Quebec Situation Update October 1, 2020
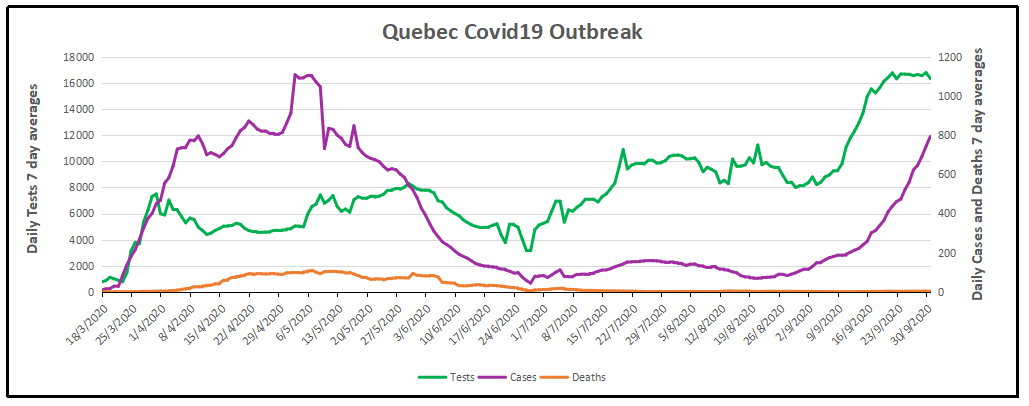
Note that testing has quadrupled since July and the number of new cases followed, especially in the last month. Meanwhile daily deaths are unchanged at less than five a day, compared to Quebec losing 186 lives every day from all causes.. Recoveries are not reported to the public, perhaps due to the large number of people testing positive but without symptoms or only mild illness and no professional treatment. The graph below estimates recoveries assuming that people not dying 28 days after a positive test can be counted as cured or in recovery.
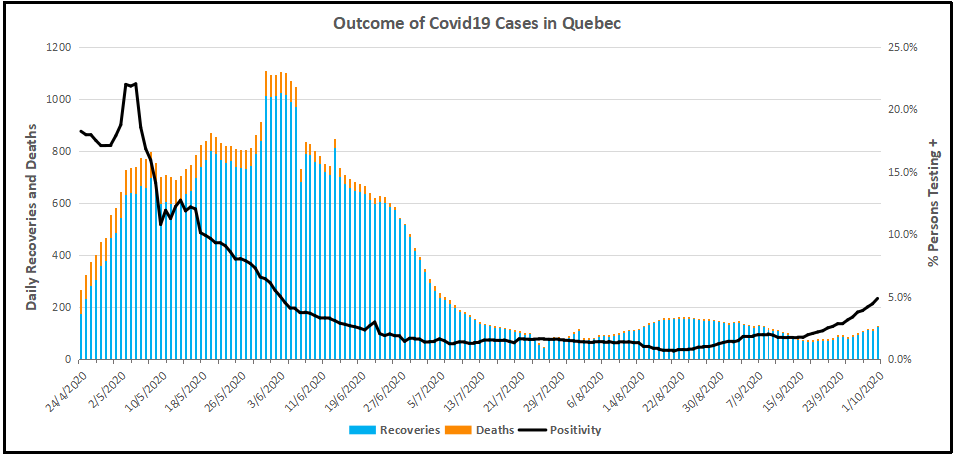
Recoveries are the number of people testing positive (misleadingly termed “cases”) minus deaths 28 days later. Obviously, the death rate was high early on, and now is barely visible. Meanwhile the Positivity rate (% of people testing positive out of all subjects) went down to 1% for several months before rising recently. Since there is a lag of 28 days, we don’t yet see the outcome of the rise in positives along with the increased testing.
Summary
Premier Legault and his medical advisors had done well up to now. The first goal was to prevent deaths, and that has been achieved. 186 Quebecers die every day from all causes, and now about 5 are dying having tested positive for SARS CV2. The other goal was to prevent overwhelming the health care system with Covid cases. This too is under control. On October 1, there were 276 patients hospitalized with covid, plus 46 in ICUs. The capacity is 1750 beds and 370 ICU beds. Since July there have been about 20 new admissions daily, offset by recoveries released from hospital.
Unfortunately, now the authorities have spooked themselves and applied a lockdown at the wrong time. Their goal has shifted to stopping new positives, which have increased because testing has quadrupled and positivity rates gone up from 1% to 5%. These are younger people who are not getting sick and certainly not dying from the virus. As many epidemiologists have said, you won’t get rid of this virus, you live with it by getting herd immunity, which leaves too few susceptible people for the virus to spread. If you kill off all the PME businesses and put people out of work, poverty and social decay will kill people, not to mention the interruption of medical treatments which save those with the real deadly diseases: cancers, heart, arteries, lungs, and so on.









 Jeffrey A. Tucker writes at AIER American Institute for Economic Research
Jeffrey A. Tucker writes at AIER American Institute for Economic Research 










 Background Post with Supporting Information
Background Post with Supporting Information